
    |     |
|
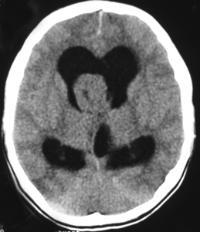
The non-contrast images demonstrate a central large mass arising in the ventricular sytem near the foramen of Munro. There is resultant obstructive hydrocephalus. The lesion has small cystic regions and enhances avidly on contrast administration. The differential diagnosis of intraventricular lesions includes:
Of these only the first two are always located at the foramen of Munro. Colloid cysts are uniformly of increased density and usually demonstrate uniform enhancement. The lesions protrude into the third ventricle inferiorly. Presentation is later in life (3rd-4th decade). The patient in this case had cutaneous manifestations consistent with Tuberous Sclerosis. Cutaneous abnormalities are not present in colloid cysts. Central neurocytomas occur in young adults and may be located near the foramen of Munro as the lesions are characteristically attached to the septum. However, these lesions are usually coarsely calcified possibly due to the frequent intratumoral haemorrhage in these cases. The other lesions listed including meningiomas (associated with skin lesions in NF-2) do not typically occur at the Foramen of Munro. In this case the location, cysts, enhancement and the presence of skin lesions (adenoma sebaceum, shagreen patches, hypo/hyperpigmented macules) are characteristic of a supendymal giant cell astrocytoma in a patient with Tuberous Sclerosis.
Approximately 15% of patients with Tuberous Sclerosis will develop a giant cell astrocytoma during their teens or early twenties. Conversely approximately 90% of patients with this type of tumour will have tuberous sclerosis. The lesion arises invariably at the Foramen of Munro and is attached to the head of the caudate, growing into the ventricles maintaining an ependymal lining. This feature contributes to the absence of intraventricular seeding. Cysts and calcifications(50%) may occur. Other cerebral stigmata of cerebral TS may or may not (as in this case) be present (eg. cortical hamartomas, supendymal nodules, white matter dysplasia) helping to differentiate from other tumours. The patient will, however, usually have other features of the disease. There is a slow progression to hydrocephalus and so symptoms may be surprisingly mild with apparent advanced disease. The tumours are Grade 1 and have a very good prognosis following resection. Registrants for the FRCR Mar 7-8th Course get emailed additional cases to review and interact with. The earlier you register the more cases you see!
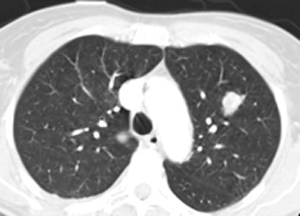
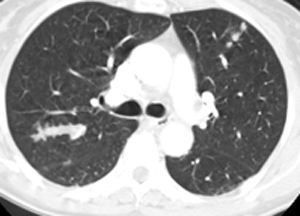
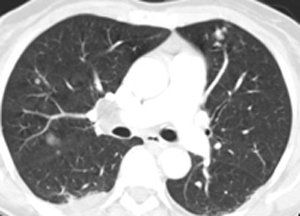
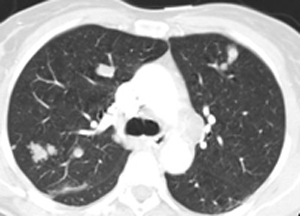
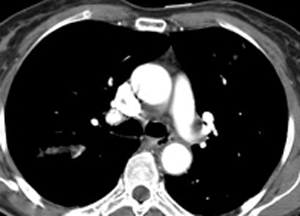
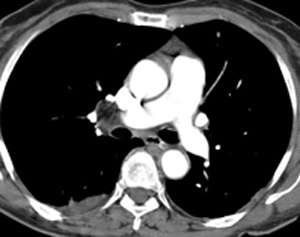
The images show multiple bony lesions. There is almost complete lytic destruction of the second middle phalanx and of the hamate, the former associated with extensive soft tissue swelling. There are multiple other areas of bone lysis mostly in a permeative pattern. The bone lesions are therefore aggressive rather than benign.
The presence of the abnormality in the hand made this case confusing and raises many diagnoses. Overall bone density is normal and there is no subperiosteal resorption or cortical tunnelling to suggest hyperparathyroidism with or without brown tumours. Gout can be very destructive but in this case there are no juxt-articular erosions or tophi to lead to this diagnosis. Enchondromas should not be so aggressive except perhaps in Maffuci’s syndrome when one should look for confirmatory phleboliths and chronic bone remodelling. Sudecks should cause more peri-articular osteopenia and bone lysis is in these regions predominantly. Myeloma does not as a rule affect the hands. If one considers the differential of multiple aggressive bone lesions irrespective of site, the differential is very short: metastases and myeloma (leaukemia and lymphoma for completeness). We will exclude infection due to multifocality. None of these affect the hands do they? Well actually the commonest cause for multifocal aggressive lesions – metastases does in one condition affect the hands – lung cancer, the correct answer in this case. Certain “rules” apply for osseous metastatic sites of involvement. The patella and mandible are for all intents and purposes never affected by metastases, the latter is affected by myeloma. Peripheral metastases in the upper limbs (beyond the elbow) and in the lower limbs (beyond the knee) are very uncommon presumably due to reduced red-marrow in these regions. Peripheral mets in the hands are almost exclusively due to lung cancer and frequently though not invariably associated with diffuse metastases elsewhere. Local symptoms of warmth and pain are common. Common sites include the distal phalanges, metacarpals, the scaphoid and lunate. In the feet lung cancer is also one of the commonest causes of metastatic disease though renal and colonic carcinoma may also metastasize to the foot, in particular the calcaneum.
62 year old man with a painful hand. What is the likeliest diagnosis?
The films demonstrate fusion of the cervical spine posterior elements. The vertebral bodies in this patient are greater in height than width (“dog” vertebrae). Even in the absence of other features that confirm the skeletally immature nature of this patient the presence of such vertebral bodies suggest a disorder occurring during development (limited weight-bearing). Commonest causes for these appearances might include Ankylosing Spondylitis, Still’s disease (JRA) and Klippel-Feil. All of these diseases would be acceptable aetiologies for the appearance in the neck, however, none of these explain the appearance of the feet.
The feet demonstrate a prominent hallux valgus deformity with microdactyly, particularly affecting the phalanges. There is partial fusion of the proximal and distal phalanges. There is no evidence of an arthropathy, bone demineralisation or diffuse bone fusion-- features that might suggest JRA. The appearances suggest a congenital aetiology. In combination these features are characteristic of fibrodysplasia ossificans progressiva. This disease density is commoner in men and often congenital with variable inheritance (sometimes autosomal dominant), often, probably more often, the disease appears as a spontaneous mutation. There is a congenital element of great toe (occasionally thumb) microdactyly, synostosis and hallux valgus that occurs in 75-90 % of cases. Even family members unaffected by other features may demonstrate this feature in 5%. Widening of the proximal femoral shaft is a less frequent finding. Presentation is usually in the first decade of life. The disease process starts in the neck, usually as painful subcutaneous nodules that enlarge progressively, coalesce and secondarily calcify or ossify (not shown in this case). These fibroblastic/myofibroblastic foci may be precipitated as the result of minor trauma or infection. The disease pathophysiology is uncertain but likely reflects abnormal collagen metabolism. Alopecia and are occasionally reported possibly related to a generalized collagen abnormality. The process extends to the cervicothoracic region and upper arms. Initial presentation is therefore often torticollis. Eventually the pelvis and more peripheral extremities may be involved. Ossification has a characteristic pattern extending cranio-caudally, dorso-ventrally and axio-appendicularly. All smooth muscle structures are spared as are the heart, diaphragm, larynx and sphincters. The process is generally one of soft tissue calcifications and ossification (tendons, ligaments, fasciae, aponeuroses) causing secondary ankylosis of joints. Hence the term pseudoexostoses, adjacent to joints. The cervical spine is an exception with progressive fusion of the posterior bony elements occurring in the second decade. Later in the disease fusion of the hip joints renders these patients immobile. Oral intake may be significantly reduced by masseter ossification (especially after dental procedures). Eventually death occurs due to restrictive respiratory failure from soft tissue ossification. However, as the disease demonstrates phenotypic heterogeneity survival in milder forms to adulthood are documented. Soft tissue calcification may be also present in other diseases (calcium disorders, dermatomyositis and calcinosis universalis/ tumoral calcinosis). It is distinguished from these conditions by the absence of trabecular bone formation (ossification). Genuine soft tissue ossification aetiologies (eg. paraplegia and burns) are distinguishable due to the absence of neck and toe involvement. Registrants for the Mar 7th-8th course receive personal cases by email to consider prior to the course, a little mental warm up. Meanwhile here is a little case to ponder for both registrants and visitors. Only one answer possible for this case. Answer coming soon....
|
From Grayscale
Latest news about Grayscale Courses, Cases to Ponder and other info Categories
All
Archives
October 2018
|







 RSS Feed
RSS Feed