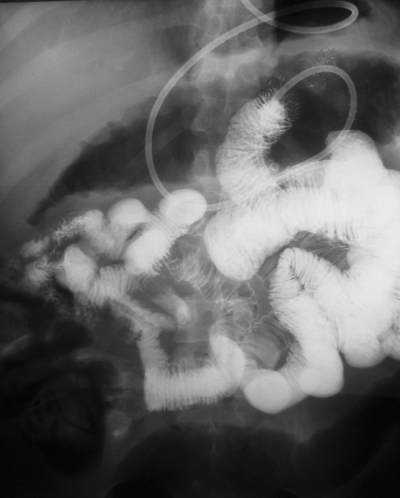
Small bowel enteroclysis study. Courtesy of Dr Aggeliki Daphnopoulou, Medical Center, P. Faliro, Athens, Greece and Vasilios Koutoulidis, from Areteion University Hospital, Athens, Greece.

|
|
|
Small bowel enteroclysis study. Courtesy of Dr Aggeliki Daphnopoulou, Medical Center, P. Faliro, Athens, Greece and Vasilios Koutoulidis, from Areteion University Hospital, Athens, Greece.
0 Comments
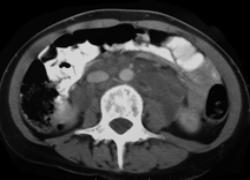
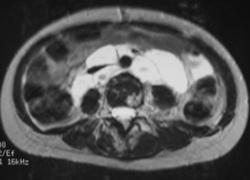
Difficult case but very characteristic appearances. What are the findings? There is a large soft tissue mass in the retroperitoneum that extends into the pelvis bilaterally and symmetrically following the lymphovascular structures to the groin. The lesion is diffusely low in density, with only minimal strands throughout. Heavily T2 weighted images demonstrate the lesion to be extremely high in T2 signal (comparable to CSF) with only thin septations. The mass demonstrates features that suggest it is “soft” in nature - the encased ureters are not obstructed. Both the CT and MR images demonstrate multiple discrete lytic lesions, very high on T2.
The differential for a low or fat density nodes in the retroperitoneum would reasonably include metastatic testicular tumour, tuberculosis, Whipple’s, MAI, TB, nerve sheath origin tumours and fat containing sarcomas. Testicular metastatic disease, with the rare exception of scrotally invading tumours, would not involve the inguinal regions as lymphatic drainage is along the blood supply to the retroperitoneum at the level of the renal veins. The presence of an enhancing uterus n the pelvis also makes this a little less likely! Whipples, MAI and TB should reasonably be excluded by the amount of abnormality present. Plexiform neurofibroma may cause a very large infiltrating mass with low CT attenuation, but the bone abnormalities would more likely be extrinsic scalloping, the T2 intensity I suspect a little lower and the symmetric pelvic involvement unusual. Nerve sheath tumours may have much the same CT/MR characteristics as a plexiform lesion but if anything be even more likely to be a focal mass. So none of the usual suspects really fit the abnormality demonstrated. If this were a child and the abnormality in the neck I suspect many would have made the diagnosis of cystic hygroma due to dilated lymphatic structures. This is a related disorder reflecting cystic dilatation of the lymphatic chains explaining the symmetric distribution of very low density, chyle containing spaces that extend down the lymphatic chains. Please note that this disease entity is distinct from lymphangioleiomyomatosis (=lymphangiomyomatosis) the cystic condition with chylous effusions condition that affects the lungs, although involvement of the lung may also occur in lymphomatosis, predominantly presenting with septal thickening or chylous effusions but not cystic lung change. Approximately two-thirds of patients with this congenital disease present with symptoms in childhood usually involving the neck, which is the site of involvement in approximately 95% of cases overall. However, adults present more often with diffuse involvement that may involve any organ system including the retroperitoneum, peritoneal cavity, chest, bones and soft tissues. The pancreas and spleen are often involved. Diffuse involvement is increasingly recognised in children too. The disease is caused by a developmental anomaly in the formation of the lymphatic system with multiple endothelial lined cystic spaces that can be demonstrated on lymphography to communicate with the lymphatic system. The process is benign but may recur locally following excision. Involvement of the bone is similar to involvement elsewhere with cystic chyle filled endothelial lined cells resulting in lucencies that may fill an entire bone. Bone overgrowth and pathological fractures are described. Presentation in children is usually with a mass. In adults presentation may be due to a mass, abdominal pain, ascites or effusions. The mass is often huge at presentation. Cystic lymphangiomatosis is probably closely related to the conditions cystic angiomatosis and cystic haemangiomatosis where there is a similar cystic proliferation of vascular endothelial spaces, causing very similar soft tissue and bone appearances (but usually with more strands of enhancement). Traumatic biopsy of lymphangiomatosis may result in erroneous diagnosis of cystic angiomatosis due to the presence of blood. Gorham’s disease (massive osteolysis of bone) may represent an aggressive variation of these diseases. This was an aunt Minnie case: Once seen never forgotten. However all the clues were there to suggest the type of tissues involved (density, location). "My motto remains"if in doubt, ask Johnny!"Johnny is an incredibly talented and exceptionally knowledgeable radiologist with an infectious enthusiasm for teaching and a fantastic personality. He approaches and explains each case, be it straightforward or the most complex rare entity, with utmost dedication and skill. To this date, I remember the detailed diagrams Johnny sketched on complex MRI physics and diagnostic algorithms during my year as a body imaging fellow and I very frequently draw upon this invaluable experience in my routine clinical practice - Johnny's teaching style is unique and has truly lasting effects! I am confident this course will equip you with the best possible tools needed for your exam; it is a golden opportunity not to be missed." - consultant and recent successful FRCR candidate
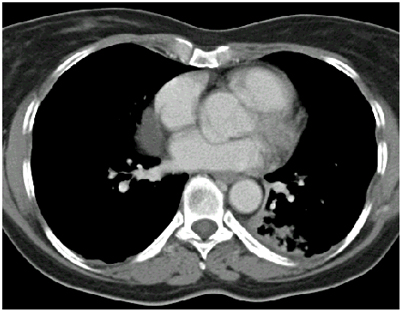
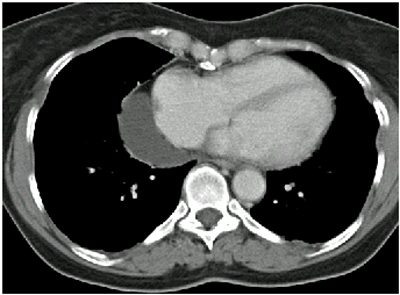
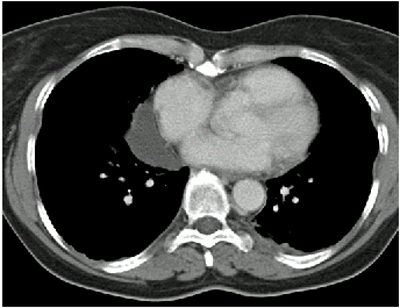
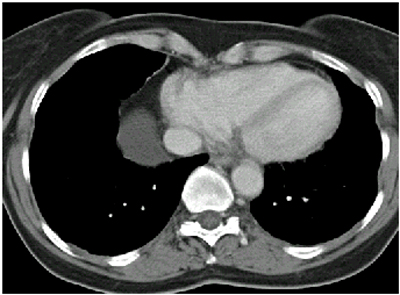
Pericardial cysts and diverticula are indistinguishable both arising from the parietal pericardium and drooping down under the weight over their contents. The contents can be confirmed on CT as fluid density although a small subset may be hyperdense. Careful technique is required to exclude erroneous densitometry due to beam hardening from intracardiac contrast. MRI, including T1 fat suppressed pre and post contrast imaging can confirm the cystic nature and absence of enhancement. Echocardiography can also be helpful but may not evaluate the lesion entirety. These lesions are usually asymptomatic although 1/3 may have a variety of non-specific symptoms. They occur more frequently in men and usually on the right side (80%). Their appearance can be vary variable on plain films depending on position and inspiration. They may appear as variable masses and cause confusion with right atrial dilatation. The key differential consideration on chest radiographs is that of a thymoma which can also extend in a mass like fashion along the right cardiac border as inferior as this. Occasionally thymomas can be cystic but usually the contents are more heterogeneous and there is a residual rim of enhancement.
"Like many other consultants who have previously been fortunate enough to be taught by Johnny Vlahos as a radiology trainee for several years, I have nothing but admiration and appreciation for the outstanding quality of the teaching he provided. Johnny is an enthusiastic, confident and empathetic individual who is committed to sharing his knowledge. This new FRCR course will undoubtedly be a success.”
"No other teacher better blends extensive rare and exotic material of "old consultants" with an abundance of cutting edge new techniques and diagnoses. The best of both worlds, delivered as only he can."
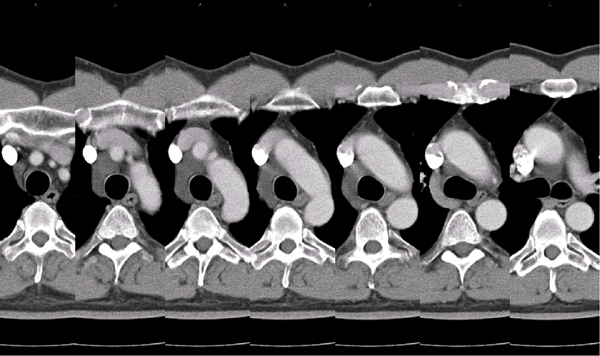
Short and sweet. There is a fluid density lesion present in the right paratracheal region. The key feature here is the absence of any peripheral soft tissue to suggest a necrotic node, homogeneous fluid attenuation and the moulding nature of this lesion to the trachea and great vessels. The diagnosis may be confirmed on multidetector CT by demonstrating communication to the typically crescentic shaped retroaortic posterior pericardial recess on 1mm reconstructed axial images or on coronal imaging (see below). Incidence is unknown, but probably far less than the 2% figure quoted in the only paper to review a series.
|
From Grayscale
Latest news about Grayscale Courses, Cases to Ponder and other info Categories
All
Archives
October 2018
|




 RSS Feed
RSS Feed