
Radiology Level: FRCR, FRCS, MRCP, ABR, EDiR, Radiology Junior +
 |  |  |
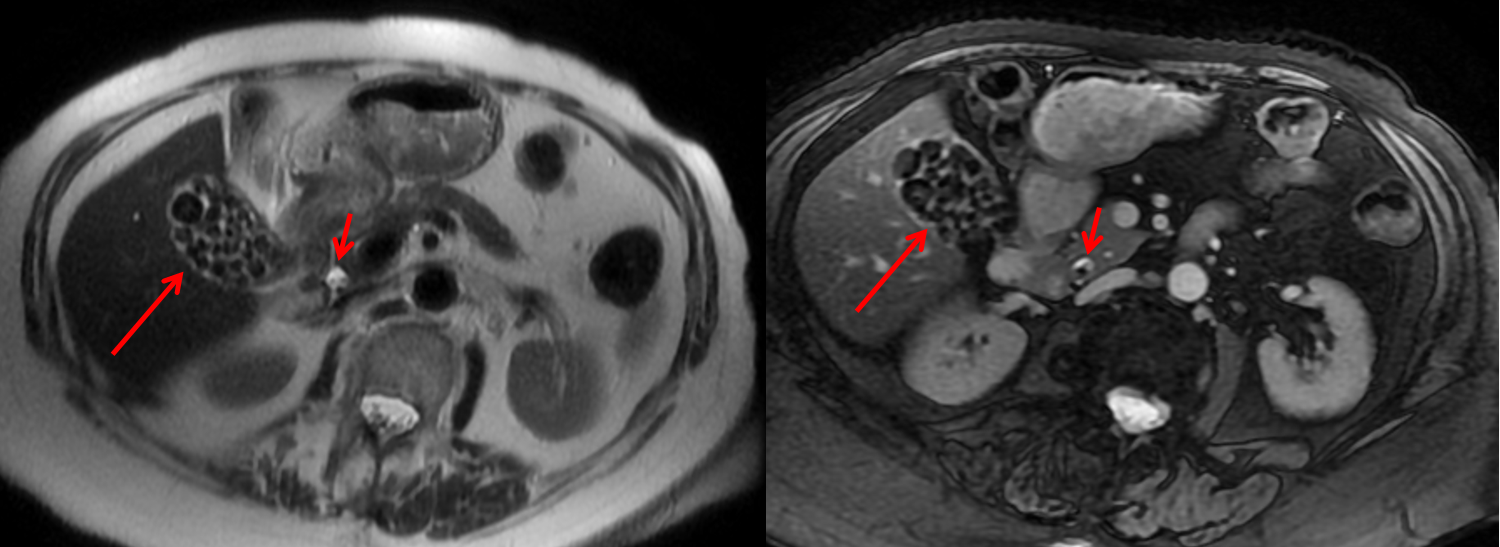
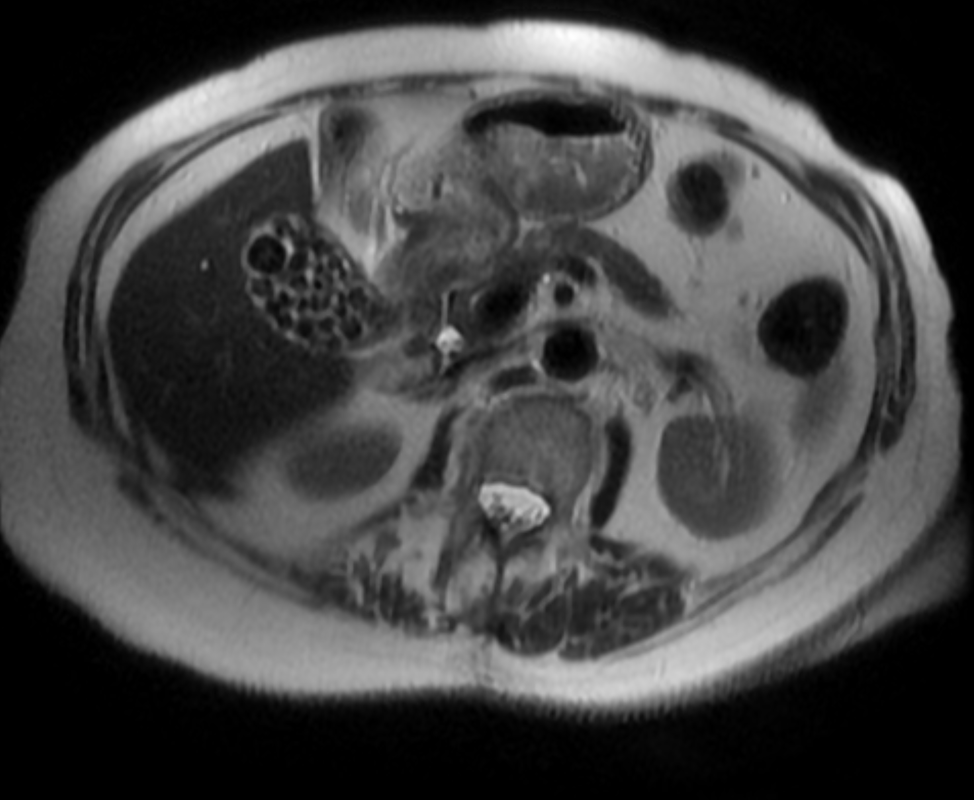
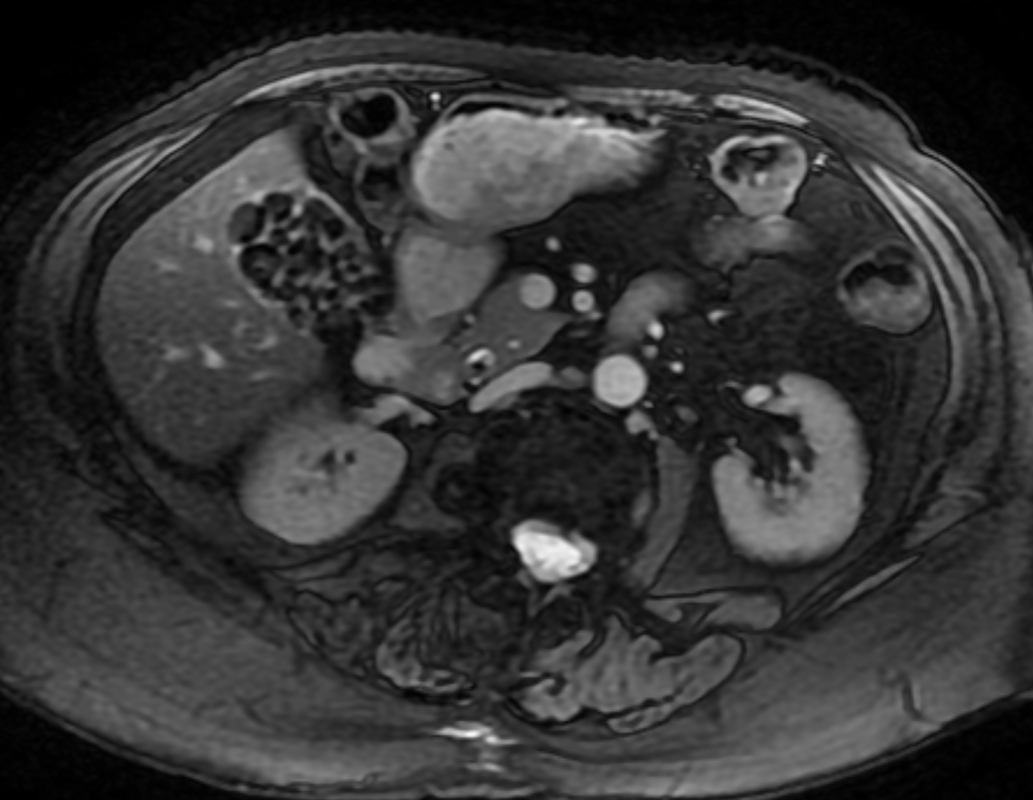
The initial images are from an MRCP (magnetic resonance cholangiopancreatography) examination. The images on the left are T2 axial images, the images on the right from a FIESTA sequence (equivalent to FISP/TRUEFISP sequence, T2 predominant-although actually ratio of T2/T1- fat suppressed, bright blood sequence) demonstrating that the gallbladder is completely packed with low signal abnormalities consistent with stones. There is no apparent gallbladder wall thickening, oedema or pericholecystic inflammation. These appearances indicate chronic gallstone disease.
It is important, however, to carefully review the remainder of the biliary tree. Hopefully, on such a review you would have also assessed the common bile duct which can be seen in the head of the pancreas (short narrow). This is mildly dilated but additionally on both the images dependent low signal abnormality can be identified consistent with bile duct stones i.e. choledocholithiasis. The presence of gallstones within the bile duct is an important parameter to indicate prior to laparoscopic surgery to ensure that the duct is cleared.
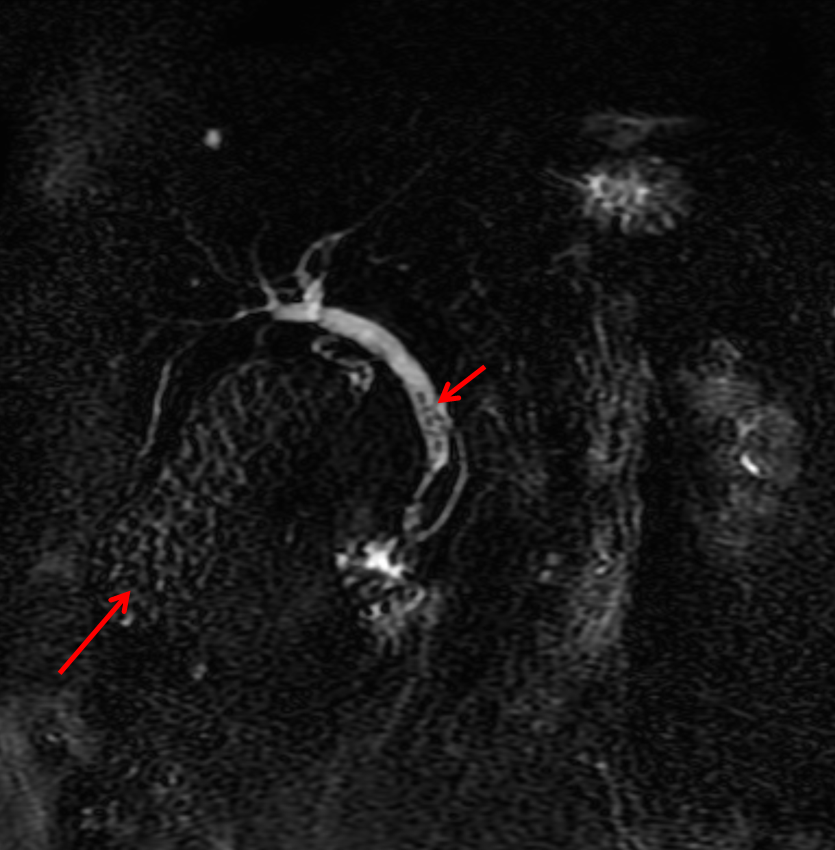
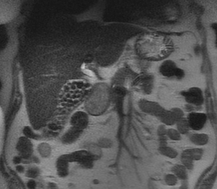
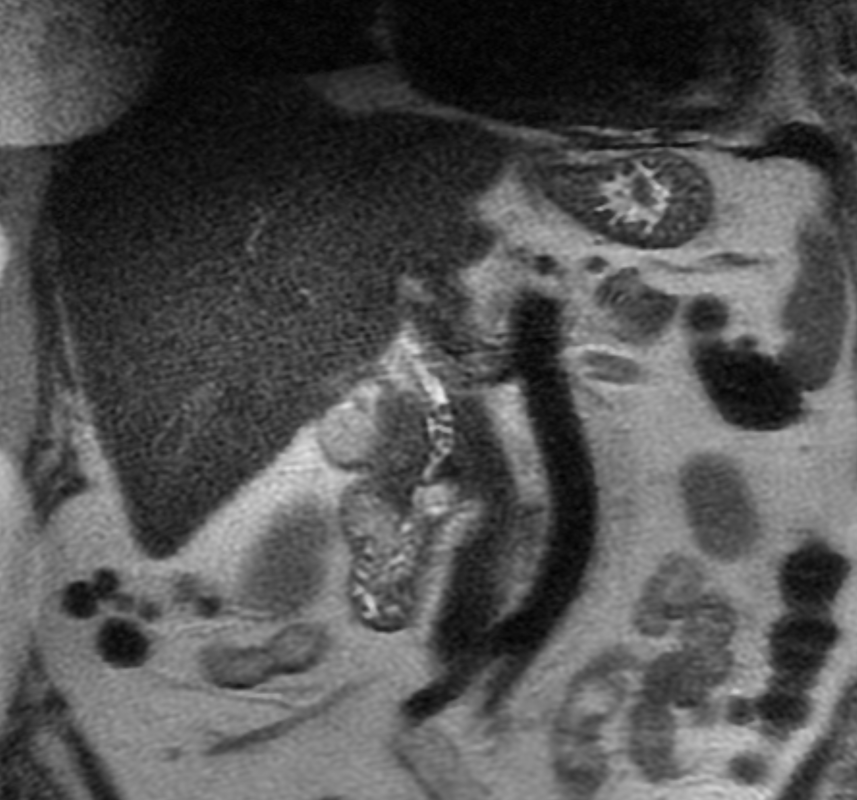
The appearances are very evident on the oblique T2-weighted radial ray projection (left). In this image it is perhaps easy to not see the gallbladder due to the loss of high T2 signal caused by multiple gallstones (long narrow). In this instance the choledocholithiasis is easily appreciated (short narrow). These are also appreciated on coronal SSFSE (single shot fast spin echo) acquired through the gallbladder and the lower biliary tree.
In identifying extrahepatic duct choledocholithiasis, particularly single stones, it is important to exclude artefact related to flow. Flow artefacts do appear central and are not consistent whereas choledocholithiasis is typically dependent and reproducible on more than one sequence. A typical site for flow artefacts is also at the crossover of the right hepatic artery over the common hepatic duct near the hepatic duct confluence.
It is important, however, to carefully review the remainder of the biliary tree. Hopefully, on such a review you would have also assessed the common bile duct which can be seen in the head of the pancreas (short narrow). This is mildly dilated but additionally on both the images dependent low signal abnormality can be identified consistent with bile duct stones i.e. choledocholithiasis. The presence of gallstones within the bile duct is an important parameter to indicate prior to laparoscopic surgery to ensure that the duct is cleared.
The appearances are very evident on the oblique T2-weighted radial ray projection (left). In this image it is perhaps easy to not see the gallbladder due to the loss of high T2 signal caused by multiple gallstones (long narrow). In this instance the choledocholithiasis is easily appreciated (short narrow). These are also appreciated on coronal SSFSE (single shot fast spin echo) acquired through the gallbladder and the lower biliary tree.
In identifying extrahepatic duct choledocholithiasis, particularly single stones, it is important to exclude artefact related to flow. Flow artefacts do appear central and are not consistent whereas choledocholithiasis is typically dependent and reproducible on more than one sequence. A typical site for flow artefacts is also at the crossover of the right hepatic artery over the common hepatic duct near the hepatic duct confluence.









 RSS Feed
RSS Feed