Let's test those skill sets by kicking it up a notch!
 |  |

|
|
|
Let's test those skill sets by kicking it up a notch!
1 Comment
Late limited availability for both dates. Additional cases for personalised feedback are already being emailed to registrants so don't miss out!
The appearances demonstrated on the AP projection demonstrate a loss of the normal radiocarpal alignment. The scaphoid is fractured and overlaps the radius. The lunate is displaced to the ulnar side and looks “odd”. There is also loss of the normal alignment of the proximal and distal row of carpal bones that should normally be roughly parallel. In this case the capitate overlaps the proximal row. These findings indicate a dislocation of the lunate or a perilunate dislocation. The lateral clarifies the anatomy better. There is loss of the normal alignment of the radius and the lunate which normally sits on the radius with the concave side facing up. In this case the lunate has tipped forward in a volar location (curved arrow). This is sometimes referred to as the “tipped teacup” appearance. These appearances in combination are referred to as a trans-scaphoid lunate dislocation. Other appearances that may be seen on the AP projection – but not seen in this case - are the “piece of pie” appearance (instead of the typical semilunar appearance) with the apex of the pie projecting distally often overlapped by the capitate. The key other consideration in these cases is that of a perilunate dislocation. Both occur due to similar mechanisms of high energy impact on an outstretched dorsiflexed hand. The appearances on the AP projection with overlap of the capitate and lunate can appear comparable. However, recall that the perilunate (“around the lunate”) dislocation is not actually a dislocation of the lunate. The difference is easily appreciated on the lateral film. In perilunate dislocation the radiolunate articulation on the lateral would be normal. The dislocation occurs above the lunate with the distal carpal bones angulated in the opposite dorsal direction. In lunate dislocation the capitate long axis remains aligned with the radius (see red line), but in perilunate dislocation the capitate angles backwards. Perilunate and lunate dislocation can –as in this case- often be associated with fractures of the scaphoid, acquiring the trans-scaphoid term. Fracture of the scaphoid may therefore also somewhat alter the typical AP and lateral appearances. With lunate dislocations it is important to consider and report the angle of rotation of the lunate. This is only 30-45° in this case but can be as much as 270°. Urgent surgical correction of dislocation and associated repair of ligaments is required although even with appropriate management premature arthritis and wrist instability is common. 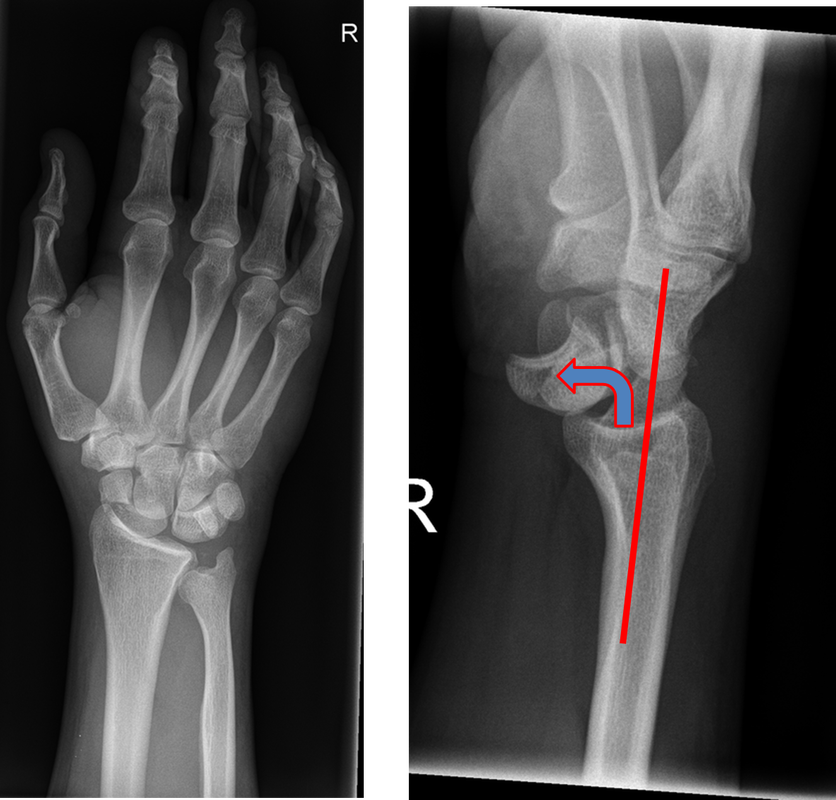 One view as they say is one view too few! Here is the lateral too!
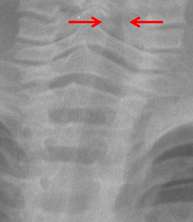
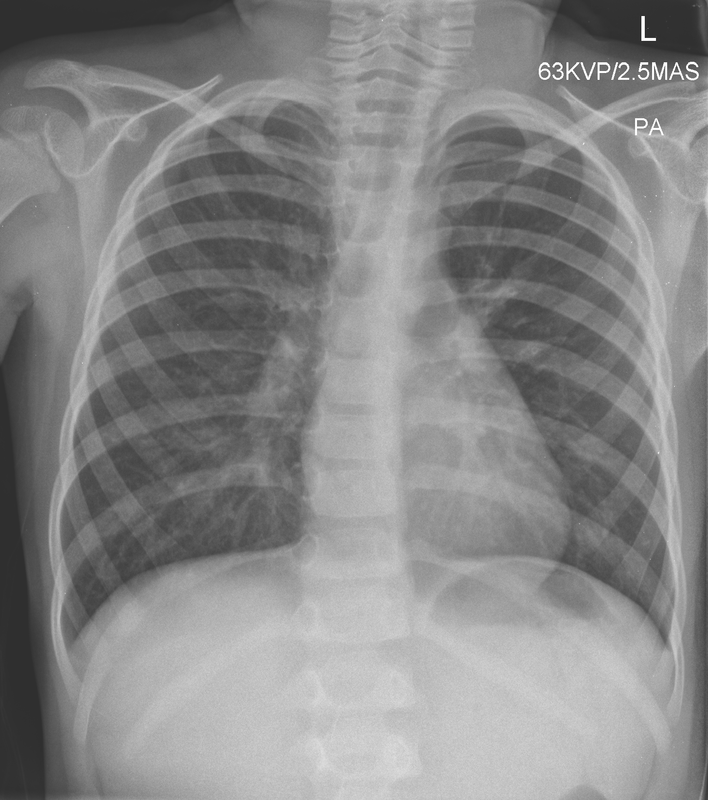
The chest radiograph is of a young child and superficially appears nearly completely normal. However, the lungs are slightly hyperinflated with mild diaphragmatic flattening. More importantly review of the subglottic tissues demonstrates absence of the normal shouldered appearance below the vocal cords. Instead there is an inverted V appearance often referred to as the “steeple sign” due to its resemblance to the steeply oriented church tower.
The “steeple sign” is an indication of subglottic oedema a common feature of croup. This oedema occurs in the first 1cm of the trachea (conus elasticus) below the true cords where the mucosa is most loosely attached and most susceptible to inflammatory oedema . Croup typically occurs in children 6 months to 3years of age usually caused by respiratory syncytial virus or parainfluenza. Indeed this child suffered a combination of croup with asthma resulting in marked inspiratory stridor and expiratory wheeze. The child deteriorated and developed a secondary lower respiratory tract infection that required intensive care hospitalization (see new image). Thankfully, the child made a complete recovery. In practice there is a quite variable appearance of the subglottic space so reporting this feature should be in the correct clinical context and ultimately the diagnosis of croup remains a clinical determination. Typically the finding is assessed on an AP radiograph of the soft tissues rather than a chest radiograph, however, can be reliably seen occasionally on chest radiographs too. As the diagnosis and management of croup should be clinical the performance of an AP radiograph of the neck soft tissues to identify this feature alone is not a sufficient indication for an AP film. The feature may occasionally also be seen in other causes of localised (epiglottis) or diffuse airway inflammation (angioneurotic oedema, bacterial tracheitis). One should also consider mucosal injuries due to thermal injury or caustic ingestion. Passwords for encrypted downloads of downloadable exams and my guidance stats-rules for Rapid Reporting have gone out to registrants by email. If you have not received yours please email [email protected]
Does it make a difference if you are a man or woman, an overseas graduate or a UK graduate? Have a look at the data.
|
From Grayscale
Latest news about Grayscale Courses, Cases to Ponder and other info Categories
All
Archives
October 2018
|





 RSS Feed
RSS Feed