
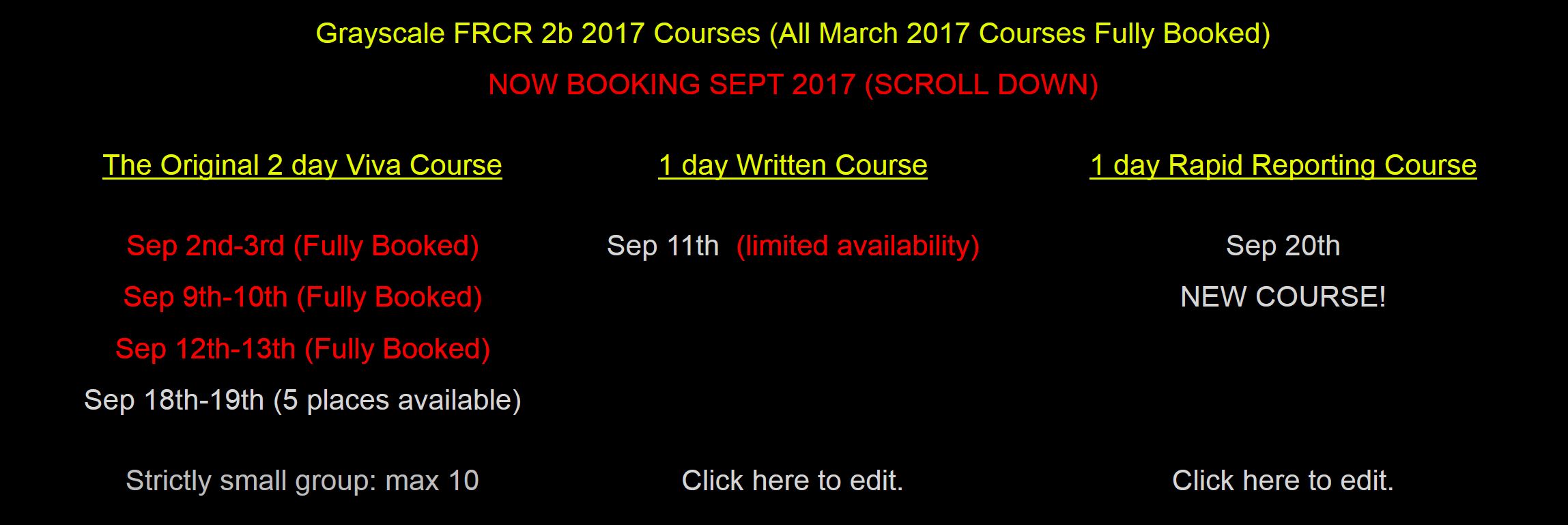
2 day original course dates (viva) all fully booked. If you are interested in a potential overflow date on 23-24 Sep please email [email protected]
Limited availability for written 1 day course (Sep 11) and Rapid Reporting 1 day courses (Sep 20) remains.
Limited availability for written 1 day course (Sep 11) and Rapid Reporting 1 day courses (Sep 20) remains.

 RSS Feed
RSS Feed