
  |   |
|
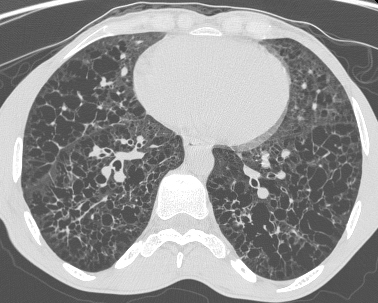
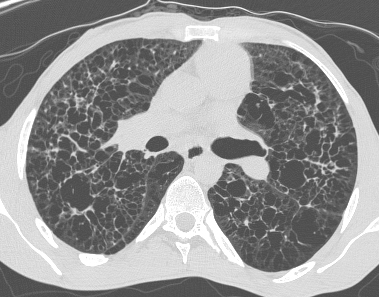
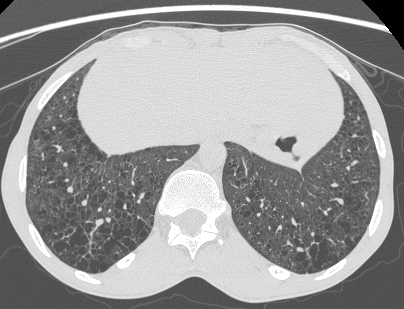
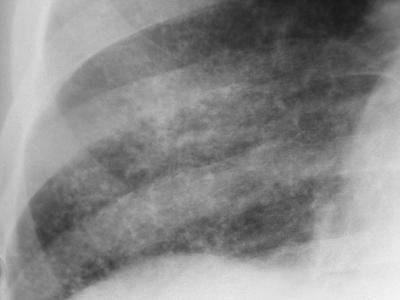
Pinpoint high density nodules are present in the lung bases and right upper lobe peripherally. The differential for pinpoint nodules is short because normal soft tissues of this density are not sufficiently radioopaque to cause appreciable discrete nodules. Remember that granulomas, varicella etc are bigger than pinpoint. So consider: High atomic number pneumoconiosis (e.g.stannosis (tin) or baritosis (barium) or silicosis- look for upper lobe predominance and dense septal lines Post lymphangiogram (not done any more) Haemosiderosis (primary: children, secondary: look for mitral valve disease) Alveolar microlithiasis (nodules usually a little bigger, often perivascular and may be outlined by black band of pericardial or pleural edges) and Heterotopic pulmonary calcification (hyperparathyroidism)- for which this appearance is characteristic. On CT these nodules are subpleural and anterior. Bone isotope imaging may show diffuse pulmonary and gastric uptake even in the absence of plain film findings. Porcelain gallbladder in same patient and calcified mesenteric nodes – postulated related to hyperparathyroidism in this patient. More characteristically an abdominal film may demonstrate nephrocalcinosis.  September Courses filling quickly:
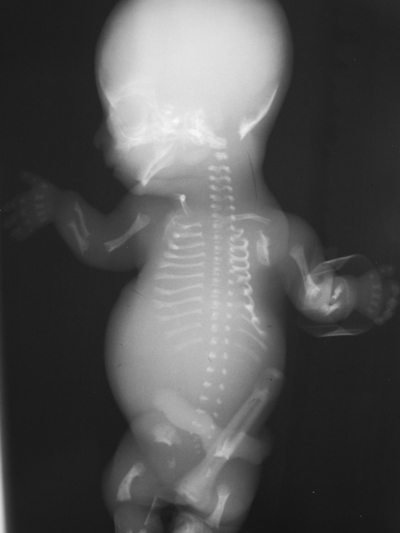
Course for Sep 12th-13th 2015 now 50% full. Greater availability for Sep 5-6th 2015 course. These courses are strictly for small groups so book early to avoid disappointment! The first thing to note in this case are the lungs and abdomen. Neither contain any air. By definition therefore this infant was unfortunately stillborn. In clinical practice this knowledge would be self-evident, however, in exams and quizzes the information must be gleaned. It is also obvious that the infant is suffering from a skeletal dysplasia. In the simplest terms therefore first consideration should be given to the commoner lethal dysplasias. These include achondrogenesis, thanatophoric dwarfism, asphyxiating thoracic dystrophy (severe), short rib-polydactyly syndromes, campomelic dysplasia and homozygous achondroplasia. Heterozygous achondroplasia, spondyloepiphyseal dysplasia and mesomelic dysplasia which are most often not lethal can be excluded prior to skeletal feature analysis. Unfortunately a few other dysplasias fall in between and are sometimes lethal including: osteogenesis imperfecta, hypophosphatasia, chondrodysplasia punctata and others. We will see, however, that features do not suggest these diagnoses.
The child demonstrates a short-limbed dwarfism with predominant shortening of the proximal limbs (rhizomelia). The chest wall is very tall and narrow, almost bell shaped and the ribs are short with flared ends. Overall bone density is normal, particularly of the calvarium and there are no fractures making hypophospahasia or osteogenesis imperfecta (the type II lethal variant) unlikely. Achondrogenesis should also be associated with calvarial and vertebral bodies that often appear absent due to poor mineralization. In this case the vertebral body epiphyses are not well seen, due to prematurity but ossification is otherwise normal. Also in achondrogenesis the chest shape is usually barrel-shaped. Campomelic dysplasia is another consideration although once again there is often poor ossification, bone shortening is not as prominent, although a bell-shape chest may occur and there is proximal bowing of the more gracile femurs, tibias and 5th digits. What other features lead to the diagnosis? Well asphyxiating thoracic dystrophy, thanatophoric dwarfism and campomelic dysplasia may all have a bell shaped narrow elongated chest. ATD and TD may also have superficially similar appearances in the pelvis – the trident appearance of the inferior acetabulum due to a inferolateral spur from the sciatic notch in ATD and the notched appearance of the acetabulum in TD due to the narrow sciatic notch demonstrated in this case. Now pay attention to the shape of the femurs. This is the key feature in this case. They are curved distally, in a so called telephone receiver configuration. This narrows the diagnosis down to one entity – thanatophoric dwarfism. Thanatophoric dwarfism or dysplasia (for those not blessed with a classical education or Greek heritage, thanatos means death, thanatophoric- carrying death) is by definition a lethal dysplasia. Death occurs due to pulmonary hypoplasia. The diagnosis may be made antenatally. Additional features not seen in this case include flattening of the vertebral bodies with more constriction of their midportions and wide intervertebral disc spaces causing an appearance likened to an inverted U or H. As seen in this case the pelvis may demonstrate small, rectangular iliac bones, small sacroiliac notches, and short and wide pubic and ischial bones. Occasionally thanatophoric dwarfism is associated with a clover-leaf skull. The condition may be occasionally indistinguishable from homozygous achondroplasia, although in such cases the diagnosis is obvious in view of both parents demonstrating the usual heterozygous form of achondroplasia. Good fun teaching KSS registrars yesterday at RSCH Guilford. Clever and engaging lot and great to catch up with old fellows now consultants.
For all but especially Grayscale Course attendees and St George's candidates!
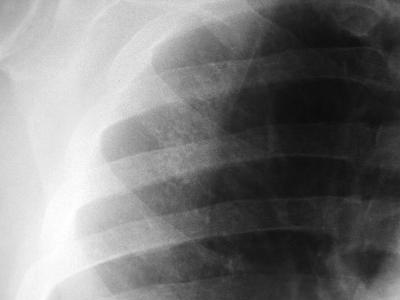
The images demonstrate a frontal and lateral projection of a barium swallow examination. The oesophagus is dilated proximally to an irregular narrowing concentric stricture with only minimal contrast seen beyond the level of obstruction. These appearances alone suggest malignancy. Oesophageal malignancy could cause these appearances, however, as we will see, there are further findings which exclude this diagnosis and confirm the correct diagnosis. The bronchial tree is particularly well visualized in this case due to senescent cartilage calcifications. However, it is noted on the frontal projection that there is an abrupt cutoff of the left main bronchus. The left hemithorax is opaque and contracted with herniation of right-sided lung parenchyma across the anterior mediastinum. The findings could be due to prior pneumonectomy or bronchial neoplasm. In the absence of surgical clips or featuers of thoracotomy the latter should be considered more likely. The additional film provided demonstrates the collapsed left lung, this image having been performed following visualization of the abnormalities on the images provided. In order to combine the findings into one malignancy diagnosis, the best unifying diagnosis is lung carcinoma with mediastinal extension or malignant nodal disease secondarily infiltrating the oesophagus. The reverse process is less likely, as mediastinal adenopathy from oesophageal carcinoma would be unlikely to peripherally extend into the left hilum without obvious abnormality on the right side. Lymphoma could bridge the anatomical distance between the oesophagus and the left main bronchus but such infiltrative disease of the oesophagus would be unusual. The findings in this case were not individually difficult, however, our eyes are conditioned to observing certain findings according to the clinical indication or examination. When presented with the findings individually it is easy to reach the correct diagnosis, yet in combination they may prove more difficult. It is always important to look at the entire film on every case. For CT this would also imply visualization of all window levels and settings. 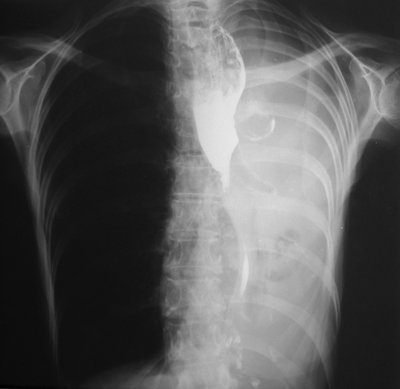 |
From Grayscale
Latest news about Grayscale Courses, Cases to Ponder and other info Categories
All
Archives
October 2018
|




 RSS Feed
RSS Feed