
This case is a complimentary case to the prior case.
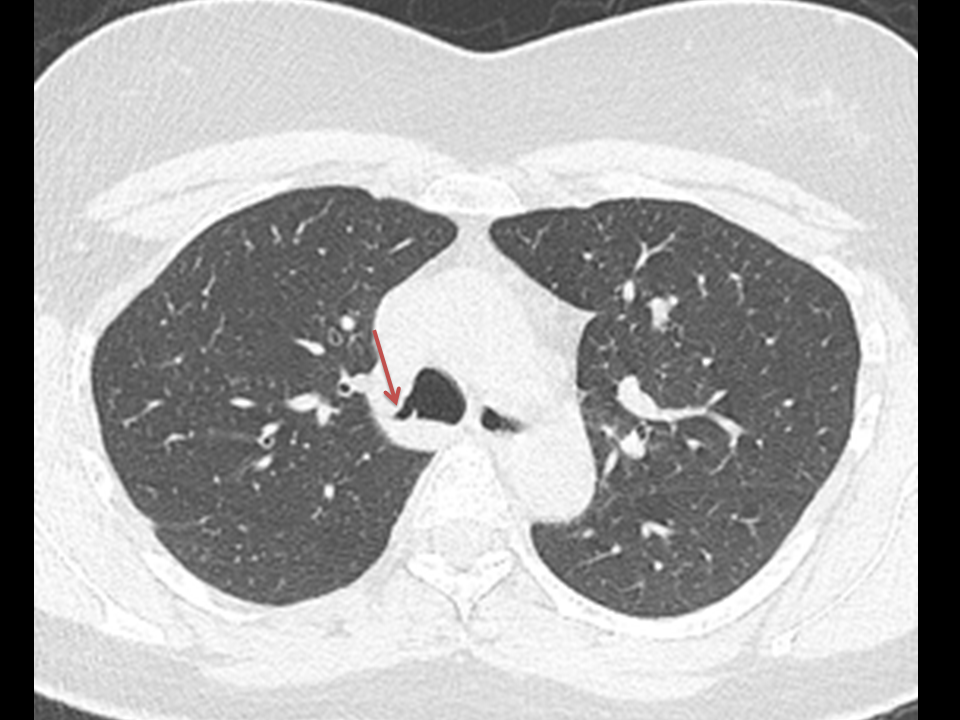
Both cases relate to congenital airways abnormalities. This is the far more common (0.5%-1%) right upper lobe bronchus arising from the trachea. This is usually an incidental finding although there are reports of associated recurrent right upper lobe infection also in the literature. In part this may be coincidental detection of the airway abnormality in people being scanned for recurrent infection but it would make sense that the narrowed airway, often arising at an acute angle as in this case, may predispose to mucoid impaction and recurrent infection. However, it should be reinforced that this is usually just an incidental finding.
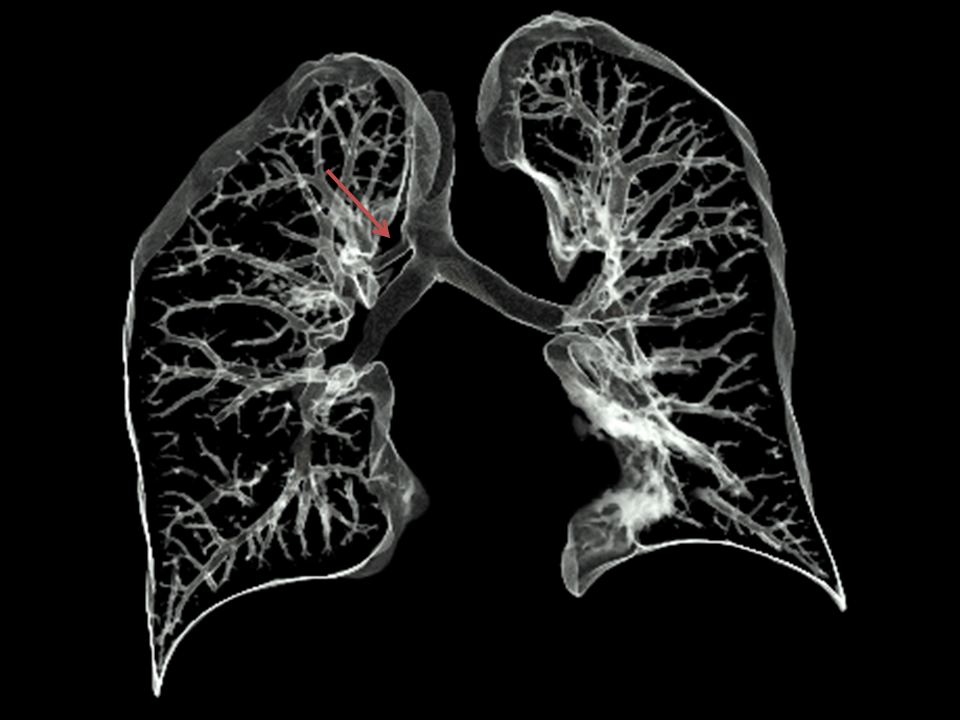
There is actually a wide variety of abnormalities that can occur in this region. Most typically in my experience and the published literature a bronchus to the apical segment of the right upper lobe arises from just beyond the origin of the right main bronchus. A separate right upper lobe bronchus supplies the anterior and posterior segments arising more distally from the right main bronchus. The next most common appearance in my experience is the one demonstrated here, an apical segmental bronchus arising from the trachea itself. Finally, origin of the entire right upper lobe bronchus from the trachea can occur although this is more uncommon. This historically has been referred to as a “pig bronchus” or “bronchus suis” although the nomenclature has been used more widely for variations in this region as above. The axial imaging clue here is that there is an additional airway above the axial plane demonstrating the tracheal bifurcation. Coronal oblique ,minimum intensity or 3D volume projections can demonstrate the anatomy beautifully for the benefit of bronchoscopists as this is a finding they should be aware of if endoscopically evaluating the patient for other reasons.
Both cases relate to congenital airways abnormalities. This is the far more common (0.5%-1%) right upper lobe bronchus arising from the trachea. This is usually an incidental finding although there are reports of associated recurrent right upper lobe infection also in the literature. In part this may be coincidental detection of the airway abnormality in people being scanned for recurrent infection but it would make sense that the narrowed airway, often arising at an acute angle as in this case, may predispose to mucoid impaction and recurrent infection. However, it should be reinforced that this is usually just an incidental finding.
There is actually a wide variety of abnormalities that can occur in this region. Most typically in my experience and the published literature a bronchus to the apical segment of the right upper lobe arises from just beyond the origin of the right main bronchus. A separate right upper lobe bronchus supplies the anterior and posterior segments arising more distally from the right main bronchus. The next most common appearance in my experience is the one demonstrated here, an apical segmental bronchus arising from the trachea itself. Finally, origin of the entire right upper lobe bronchus from the trachea can occur although this is more uncommon. This historically has been referred to as a “pig bronchus” or “bronchus suis” although the nomenclature has been used more widely for variations in this region as above. The axial imaging clue here is that there is an additional airway above the axial plane demonstrating the tracheal bifurcation. Coronal oblique ,minimum intensity or 3D volume projections can demonstrate the anatomy beautifully for the benefit of bronchoscopists as this is a finding they should be aware of if endoscopically evaluating the patient for other reasons.
 |  |
 RSS Feed
RSS Feed