
 | 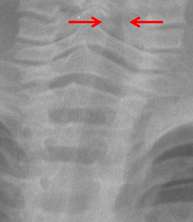 |  |
The chest radiograph is of a young child and superficially appears nearly completely normal. However, the lungs are slightly hyperinflated with mild diaphragmatic flattening. More importantly review of the subglottic tissues demonstrates absence of the normal shouldered appearance below the vocal cords. Instead there is an inverted V appearance often referred to as the “steeple sign” due to its resemblance to the steeply oriented church tower.
The “steeple sign” is an indication of subglottic oedema a common feature of croup. This oedema occurs in the first 1cm of the trachea (conus elasticus) below the true cords where the mucosa is most loosely attached and most susceptible to inflammatory oedema . Croup typically occurs in children 6 months to 3years of age usually caused by respiratory syncytial virus or parainfluenza. Indeed this child suffered a combination of croup with asthma resulting in marked inspiratory stridor and expiratory wheeze. The child deteriorated and developed a secondary lower respiratory tract infection that required intensive care hospitalization (see new image). Thankfully, the child made a complete recovery.
In practice there is a quite variable appearance of the subglottic space so reporting this feature should be in the correct clinical context and ultimately the diagnosis of croup remains a clinical determination. Typically the finding is assessed on an AP radiograph of the soft tissues rather than a chest radiograph, however, can be reliably seen occasionally on chest radiographs too. As the diagnosis and management of croup should be clinical the performance of an AP radiograph of the neck soft tissues to identify this feature alone is not a sufficient indication for an AP film. The feature may occasionally also be seen in other causes of localised (epiglottis) or diffuse airway inflammation (angioneurotic oedema, bacterial tracheitis). One should also consider mucosal injuries due to thermal injury or caustic ingestion.
The “steeple sign” is an indication of subglottic oedema a common feature of croup. This oedema occurs in the first 1cm of the trachea (conus elasticus) below the true cords where the mucosa is most loosely attached and most susceptible to inflammatory oedema . Croup typically occurs in children 6 months to 3years of age usually caused by respiratory syncytial virus or parainfluenza. Indeed this child suffered a combination of croup with asthma resulting in marked inspiratory stridor and expiratory wheeze. The child deteriorated and developed a secondary lower respiratory tract infection that required intensive care hospitalization (see new image). Thankfully, the child made a complete recovery.
In practice there is a quite variable appearance of the subglottic space so reporting this feature should be in the correct clinical context and ultimately the diagnosis of croup remains a clinical determination. Typically the finding is assessed on an AP radiograph of the soft tissues rather than a chest radiograph, however, can be reliably seen occasionally on chest radiographs too. As the diagnosis and management of croup should be clinical the performance of an AP radiograph of the neck soft tissues to identify this feature alone is not a sufficient indication for an AP film. The feature may occasionally also be seen in other causes of localised (epiglottis) or diffuse airway inflammation (angioneurotic oedema, bacterial tracheitis). One should also consider mucosal injuries due to thermal injury or caustic ingestion.
 RSS Feed
RSS Feed