
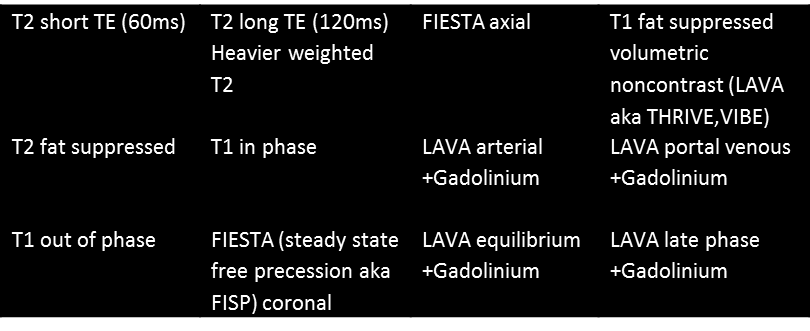
The sequences depicted are as follows:
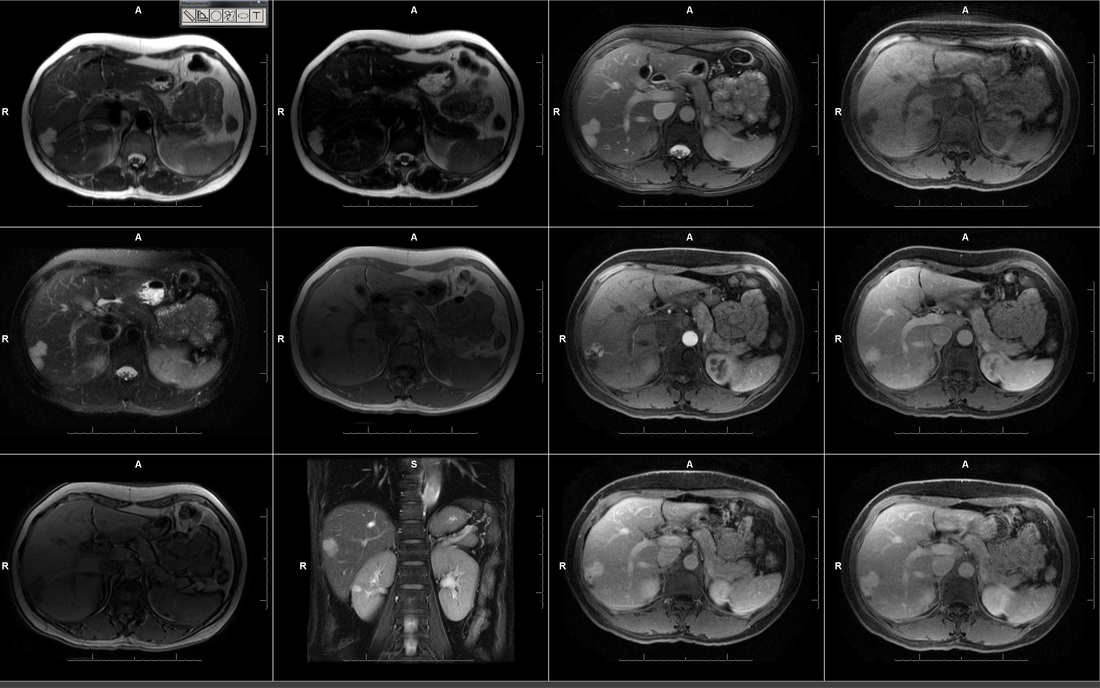
These are classical diagnostic images of a haemangioma. The initial images demonstrate that there is a lobular subcapsular lesion in the right liver lobe. This demonstrates moderately elevated T2 signal that is more conspicuous on the heavier T2 weighted images. Note that this does not mean measurably brighter, just more conspicuous in comparison to the background hepatic parenchyma which is more suppressed on heavier T2 weighted images. This feature of increasing conspicuousness on heavier T2 weighted images is an appearance that is indicative of a benign lesion.
The lesion is slightly more apparent on T2 fat suppressed images. The FIESTA sequences are not pure T2 sequences but a ratio of T2/T1. However, in general these sequences are rapidly acquired resulting in higher resolution “surrogate” T2 lesions. The lesion demonstrates low T1 signal intensity. There is no loss of signal of the lesion or the background parenchyma on out of phase images.
The T1 fat suppressed volumetric images that can be acquired in multiple phases before and after Gadolinium administration are the key for evaluation of any focal liver lesion. These demonstrate nodular peripheral arterial enhancement. This becomes progressively more prominent in later phases of evaluation with “centripetal” in filling of the hepatic lesion. By the final image the lesion is completely in-filled, a finding that is not essential for the diagnosis as many haemagiomas are centrally fibrosed and may not fill in centrally or be very delayed. The demonstration of the peripheral nodular interrupted enhancement is sufficient for diagnosis and differentiates lesions from the continuous rim enhancement of malignant lesions.
Note also that the haemangioma follows the blood pool in every phase of enhancement. This is an often stated characteristic of haemangiomas that can be difficult to understand as stated. I prefer the statement that “the lesion follows the dominant vascular phase at every time point”. For example, in the arterial phase the nodular enhancement is the same as the arteries and in later phases is equivalent to the portal veins, and the hepatic veins. This can be a very helpful feature for atypical or small lesions.
The lesion is slightly more apparent on T2 fat suppressed images. The FIESTA sequences are not pure T2 sequences but a ratio of T2/T1. However, in general these sequences are rapidly acquired resulting in higher resolution “surrogate” T2 lesions. The lesion demonstrates low T1 signal intensity. There is no loss of signal of the lesion or the background parenchyma on out of phase images.
The T1 fat suppressed volumetric images that can be acquired in multiple phases before and after Gadolinium administration are the key for evaluation of any focal liver lesion. These demonstrate nodular peripheral arterial enhancement. This becomes progressively more prominent in later phases of evaluation with “centripetal” in filling of the hepatic lesion. By the final image the lesion is completely in-filled, a finding that is not essential for the diagnosis as many haemagiomas are centrally fibrosed and may not fill in centrally or be very delayed. The demonstration of the peripheral nodular interrupted enhancement is sufficient for diagnosis and differentiates lesions from the continuous rim enhancement of malignant lesions.
Note also that the haemangioma follows the blood pool in every phase of enhancement. This is an often stated characteristic of haemangiomas that can be difficult to understand as stated. I prefer the statement that “the lesion follows the dominant vascular phase at every time point”. For example, in the arterial phase the nodular enhancement is the same as the arteries and in later phases is equivalent to the portal veins, and the hepatic veins. This can be a very helpful feature for atypical or small lesions.
 RSS Feed
RSS Feed