
 |  |
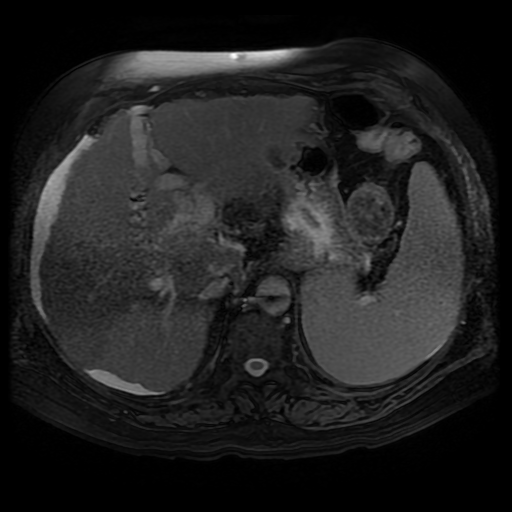 | 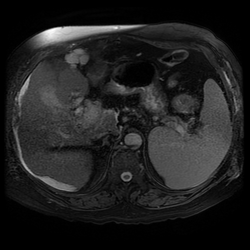 | 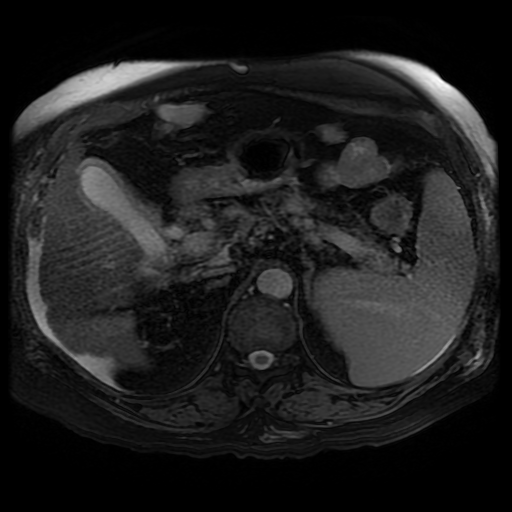 |
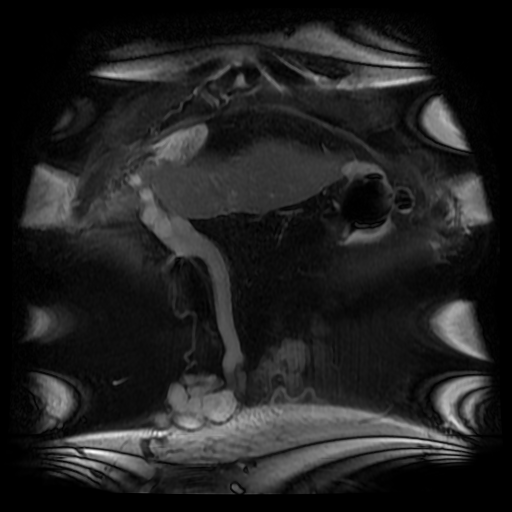
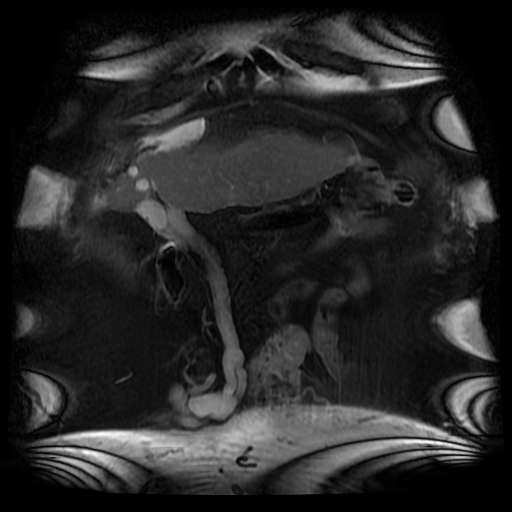
This is a single non-contrast coronal image from an MRI examination (Coronal FIESTA). This is sufficient to make the clinical diagnosis, although more reference images are presented for anatomical completeness. There is a large venous structure arising from the anterior surface of the liver near the falciform ligament. This extends inferiorly into the midline where it ends in a tangle of vessels near the umbilicus. These appearances are characteristic of “Caput Medusae” the serpent head of the mythical Gorgon Medusa. These findings reflect porto-systemic circulation anastomoses developing in a patient with portal hypertension due to chronic liver disease with cirrhosis.
The caput develops due to recanalization of the para-umbilical vein in the falciform ligament, a structure that usually occludes in the second week of life. As with all collateral or variceal vessels identified at CT, MRI or ultrasound it is critical to the diagnosis to consider the direction of flow and what the objective of the varices is. The object of this recanalization is to divert portal venous blood away from the high pressure liver. As the venous vessels radiate from the umbilicus they anastomose with systemic veins diverting portal venous flow. Rarely the inverse direction of flow can be seen in patients with inferior vena cava obstruction. Although recanalization of the portal vein is not uncommon a fully formed Caput medusae is an indication of severe portal hypertension.
More common attempted porto-systemic anastomoses include gastro-oesophageal varices (anastomosing with the systemic lower oesophageal veins) or lienorenal shunts (splenic veins anastomosing with the left renal vein). Portosystemic shunts can also occur around the rectum due to anastomosis of the superior rectal veins (draining to the portal venous system) and inferior rectal/anal veins anastomosing to the internal iliac circulation, although these are also uncommon and seen in very advanced cases.
The caput develops due to recanalization of the para-umbilical vein in the falciform ligament, a structure that usually occludes in the second week of life. As with all collateral or variceal vessels identified at CT, MRI or ultrasound it is critical to the diagnosis to consider the direction of flow and what the objective of the varices is. The object of this recanalization is to divert portal venous blood away from the high pressure liver. As the venous vessels radiate from the umbilicus they anastomose with systemic veins diverting portal venous flow. Rarely the inverse direction of flow can be seen in patients with inferior vena cava obstruction. Although recanalization of the portal vein is not uncommon a fully formed Caput medusae is an indication of severe portal hypertension.
More common attempted porto-systemic anastomoses include gastro-oesophageal varices (anastomosing with the systemic lower oesophageal veins) or lienorenal shunts (splenic veins anastomosing with the left renal vein). Portosystemic shunts can also occur around the rectum due to anastomosis of the superior rectal veins (draining to the portal venous system) and inferior rectal/anal veins anastomosing to the internal iliac circulation, although these are also uncommon and seen in very advanced cases.

The Caput Medusae refers to the serpent head of the Gorgon Medusa. Looking at Medusa’s directly would petrify onlookers. The image below demonstrates a Canova (1804-1806) sculpture from the Metropolitan Museum of Art in New York City. This demonstrates Perseus beheading the Gordon Medusa. In this depicted version of mythology Perseus used the invisibility cap of Hades to behead her. More commonly it is stated that Perseus slayed Medusa by viewing her reflection in a bronze shield provided by Athena. From Medusa’s blood arose Chrysaor (a golden giant) and Pegasus (the winged horse)! Radiology and Mythology on a Sunday morning!
 RSS Feed
RSS Feed