
Classic Case: Radiology Level - Challenge ++++, FRCR, EDiR, ABR, MRCP
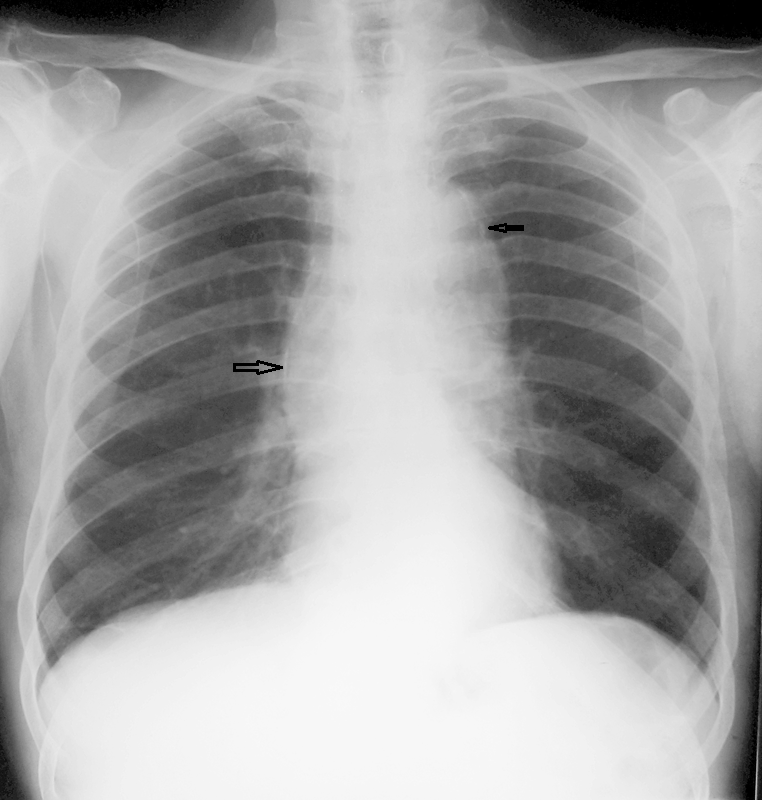 |  |
A chest radiograph and an AP lumbar spine radiograph are provided. The chest radiograph demonstrates unfolding of the thoracic aorta which may be aneurysmal although this can be difficult to determine on a plain radiograph alone. There is fine linear calcification running along the right lateral margin of the mediastinum (large arrow), identifying the lateral aspect of the aortic arch. This extends in a continuous fashion to the coarsely calcified ligamentum arteriosum in the AP window (small arrow). There is no coarse calcification of the aorta. The heart size is normal. The lungs are clear.
The AP radiograph of the lumbar spine demonstrate a right total hip replacement and a short segment scoliosis of the mid lumbar spine associated with sclerosis and some fragmentation of the concave aspect as well as new bone formation and loss of normal orientation. There are no congenital variations in this region.
There are several ways in which we can approach the interpretation of these images. A short segment scoliosis has a relatively limited differential. This includes congenital variations such as hemivertebrae related to failures of segmentation such as occurring patients with neurofibromatosis or VACTERL. None of these are present here. Post traumatic appearances can result in short segment scoliosis, however, again not demonstrated here. Tuberculous destruction can result in discitis with partial collapse, however, the endplates, typically destroyed in tuberculous discitis, are well preserved in this instance and the abnormality extends over several levels. Finally one can consider the possibility of a neuropathic (Charcot)spine which is the best fit for the current appearance. Much like other joints a neuropathic spine is associated with the 4 Ds (density, destruction, debris, deformity/dislocation). Causes of a neuropathic spine include spinal cord injury, diabetes and tabes dorsalis (syphilitic).
The most common current cause of a Charcot spine is diabetes, however, in this instance the chest radiograph provides an additional clue. The ascending aortic dilatation and fine ascending aortic peripheral calcification, in contradistinction to the coarse thick calcifications of atherosclerotic aortas arising near the aortic isthmus are typical of syphilitic aortitis. This is the unifying diagnosis in this case–tertiary syphilis with syphilitic aortitis and tabes dorsalis.
Syphilitic aortitis (previously termed luetic aneurysm/aortitis) is a tertiary manifestation of syphilis infection. This is an adventitial disease process resulting in obliterative endarteritis of the vasa vasora resulting in ischaemic injury of the adventitial/media which may progress to aneurysm formation or fine peripheral calcification. Dissection is unusual due to the fibrosis of the medial layer. Coronary calcification, or involvement of the aortic root may also occur. At CT asymmetrical aortic sinus involvement or "tree bark" intimal calcifications can be demonstrated. The disease process is now rare in the Western World due to the reduction of syphilitic infections following introduction of penicillin.
Tabes dorsalis is a form of tertiary neurosyphilis. These presents with dorsal column/nerve root symptomatology relating to weakness and abnormal gait related to lack of proprioception with sensory ataxia (tabetic gait) that as in this case may predispose to falls. Lightening-like paraesthesia pains can occur with altered sensation from joints result in degeneration, as in this case with a right hip replacement. The lower limbs demonstrate hypotonia and diminished reflexes. The differential diagnosis includes other demyelinating pathologies of the cord including multiple sclerosis, transverse myelitis, HIV, Vitamin B12 deficiency resulting in subacute combined degeneration, and focal neoplasms.
This is a classic radiological interpretation to enjoy. A bonus features seen in some cases is calcification of injections in the buttocks due to Bimuth injections predating penicillin treatment.
The AP radiograph of the lumbar spine demonstrate a right total hip replacement and a short segment scoliosis of the mid lumbar spine associated with sclerosis and some fragmentation of the concave aspect as well as new bone formation and loss of normal orientation. There are no congenital variations in this region.
There are several ways in which we can approach the interpretation of these images. A short segment scoliosis has a relatively limited differential. This includes congenital variations such as hemivertebrae related to failures of segmentation such as occurring patients with neurofibromatosis or VACTERL. None of these are present here. Post traumatic appearances can result in short segment scoliosis, however, again not demonstrated here. Tuberculous destruction can result in discitis with partial collapse, however, the endplates, typically destroyed in tuberculous discitis, are well preserved in this instance and the abnormality extends over several levels. Finally one can consider the possibility of a neuropathic (Charcot)spine which is the best fit for the current appearance. Much like other joints a neuropathic spine is associated with the 4 Ds (density, destruction, debris, deformity/dislocation). Causes of a neuropathic spine include spinal cord injury, diabetes and tabes dorsalis (syphilitic).
The most common current cause of a Charcot spine is diabetes, however, in this instance the chest radiograph provides an additional clue. The ascending aortic dilatation and fine ascending aortic peripheral calcification, in contradistinction to the coarse thick calcifications of atherosclerotic aortas arising near the aortic isthmus are typical of syphilitic aortitis. This is the unifying diagnosis in this case–tertiary syphilis with syphilitic aortitis and tabes dorsalis.
Syphilitic aortitis (previously termed luetic aneurysm/aortitis) is a tertiary manifestation of syphilis infection. This is an adventitial disease process resulting in obliterative endarteritis of the vasa vasora resulting in ischaemic injury of the adventitial/media which may progress to aneurysm formation or fine peripheral calcification. Dissection is unusual due to the fibrosis of the medial layer. Coronary calcification, or involvement of the aortic root may also occur. At CT asymmetrical aortic sinus involvement or "tree bark" intimal calcifications can be demonstrated. The disease process is now rare in the Western World due to the reduction of syphilitic infections following introduction of penicillin.
Tabes dorsalis is a form of tertiary neurosyphilis. These presents with dorsal column/nerve root symptomatology relating to weakness and abnormal gait related to lack of proprioception with sensory ataxia (tabetic gait) that as in this case may predispose to falls. Lightening-like paraesthesia pains can occur with altered sensation from joints result in degeneration, as in this case with a right hip replacement. The lower limbs demonstrate hypotonia and diminished reflexes. The differential diagnosis includes other demyelinating pathologies of the cord including multiple sclerosis, transverse myelitis, HIV, Vitamin B12 deficiency resulting in subacute combined degeneration, and focal neoplasms.
This is a classic radiological interpretation to enjoy. A bonus features seen in some cases is calcification of injections in the buttocks due to Bimuth injections predating penicillin treatment.
 RSS Feed
RSS Feed