
Level: MRCP, ABR, EDiR, FRCR, Radiology Junior +
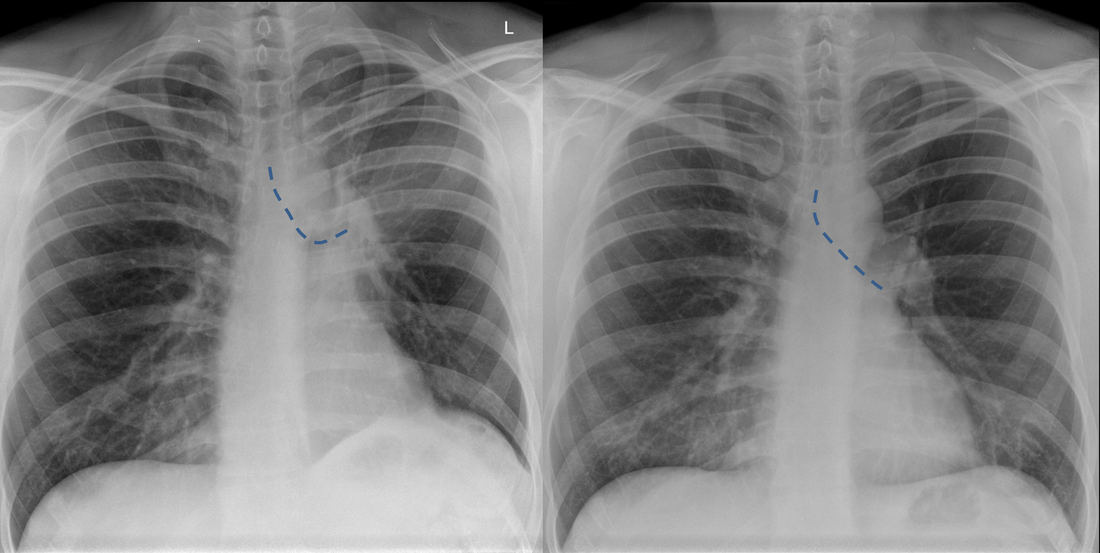
| Current | 6 weeks Prior |
The current chest radiograph is clearly abnormal, the prior chest radiograph provided for comparison was normal. The current chest radiograph demonstrates left perihilar opacity denser centrally, fading towards the periphery. There is a retained lucency medially, lateral to the aortic arch. The left hilum is elevated. Note also that the left main bronchus (dotted line) is now horizontal, compared to the oblique normal orientation on the prior film. The left hemidiaphragm is slightly more elevated and the cardiac silhouette slightly more displaced to the left, not now protruding to the right of the spine. These characteristic appearances are all indicative of volume loss in the upper left hemithorax, specifically left upper lobe collapse.
In left upper lobe collapse, the left upper lobe collapses anteriorly. This anterior movement of the collapsed lung is greater peripherally and more restrained by the hilar attachment medially. So centrally density is retained and peripherally this fades. When the lung is minimally collapsed the entire left lung may demonstrate diffuse opacity through which vessels are still seen in the lower lobe. These appearances are the so called “veil like” opacity. As the collapse progresses, as in this case, the opacity contracts towards the hilum. Paradoxically, the opacity generated by the collapse reduces as the severity of the collapse increases. In these instances it is important to assess ancillary features of volume loss to differentiate the perihilar opacity of collapse from a mass.
In this case the loss of volume in the left hemithorax is supported by the cardiomediastinal shift and the minor elevation of the left hemidiaphragm. In general terms upper lobe collapses tend to cause shift of the upper mediastinum whereas lower lobe collapses cause greater shift of the lower mediastinum and heart, although, as in this case, that is inconsistent. Tenting of the diaphragm, sometimes termed a juxtaphrenic peak, can also occur due to attachments of the hilum to the inferior pleural surface via an inferior accessory fissure or less frequently an inferiorly extending inferior pulmonary ligament. Generally, unless dealing with extreme long-standing fibrotic upper lobe collapse, significant elevation of the hemidiaphragm is unusual. If there is significant elevation it is important to consider that the collapse is due to a malignancy with infiltration of the phrenic nerve.
The upper lobe collapse is confirmed by elevation of the hilum and loss of clarity of the previously visible left pulmonary artery. The horizontal nature of the bronchus, further adds weight to the upper volume loss. Finally, a specific feature supports the left upper lobe collapse. That is the peri-aortic lucency, often termed the “Lűftsichel sign” (sickle of air). This is appearance is due to superior herniation of compensatorily hyperinflated left lower lobe lung parenchyma medial to the collapsed left upper lobe.
In this case the collapse was due to an entirely endobronchial carcinoid tumour with none of the opacity visualised in the perihilar region due to tumour but all due to left upper lobe collapse.
In left upper lobe collapse, the left upper lobe collapses anteriorly. This anterior movement of the collapsed lung is greater peripherally and more restrained by the hilar attachment medially. So centrally density is retained and peripherally this fades. When the lung is minimally collapsed the entire left lung may demonstrate diffuse opacity through which vessels are still seen in the lower lobe. These appearances are the so called “veil like” opacity. As the collapse progresses, as in this case, the opacity contracts towards the hilum. Paradoxically, the opacity generated by the collapse reduces as the severity of the collapse increases. In these instances it is important to assess ancillary features of volume loss to differentiate the perihilar opacity of collapse from a mass.
In this case the loss of volume in the left hemithorax is supported by the cardiomediastinal shift and the minor elevation of the left hemidiaphragm. In general terms upper lobe collapses tend to cause shift of the upper mediastinum whereas lower lobe collapses cause greater shift of the lower mediastinum and heart, although, as in this case, that is inconsistent. Tenting of the diaphragm, sometimes termed a juxtaphrenic peak, can also occur due to attachments of the hilum to the inferior pleural surface via an inferior accessory fissure or less frequently an inferiorly extending inferior pulmonary ligament. Generally, unless dealing with extreme long-standing fibrotic upper lobe collapse, significant elevation of the hemidiaphragm is unusual. If there is significant elevation it is important to consider that the collapse is due to a malignancy with infiltration of the phrenic nerve.
The upper lobe collapse is confirmed by elevation of the hilum and loss of clarity of the previously visible left pulmonary artery. The horizontal nature of the bronchus, further adds weight to the upper volume loss. Finally, a specific feature supports the left upper lobe collapse. That is the peri-aortic lucency, often termed the “Lűftsichel sign” (sickle of air). This is appearance is due to superior herniation of compensatorily hyperinflated left lower lobe lung parenchyma medial to the collapsed left upper lobe.
In this case the collapse was due to an entirely endobronchial carcinoid tumour with none of the opacity visualised in the perihilar region due to tumour but all due to left upper lobe collapse.
 RSS Feed
RSS Feed