
Level: EDiR, ABR, FRCR Radiology Mid-Level ++
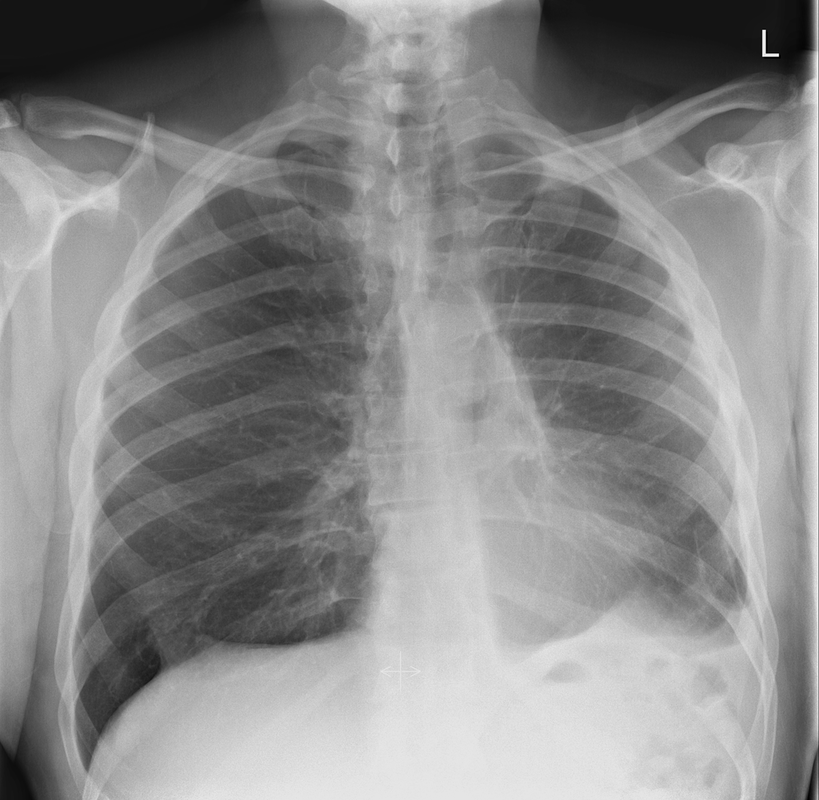 | 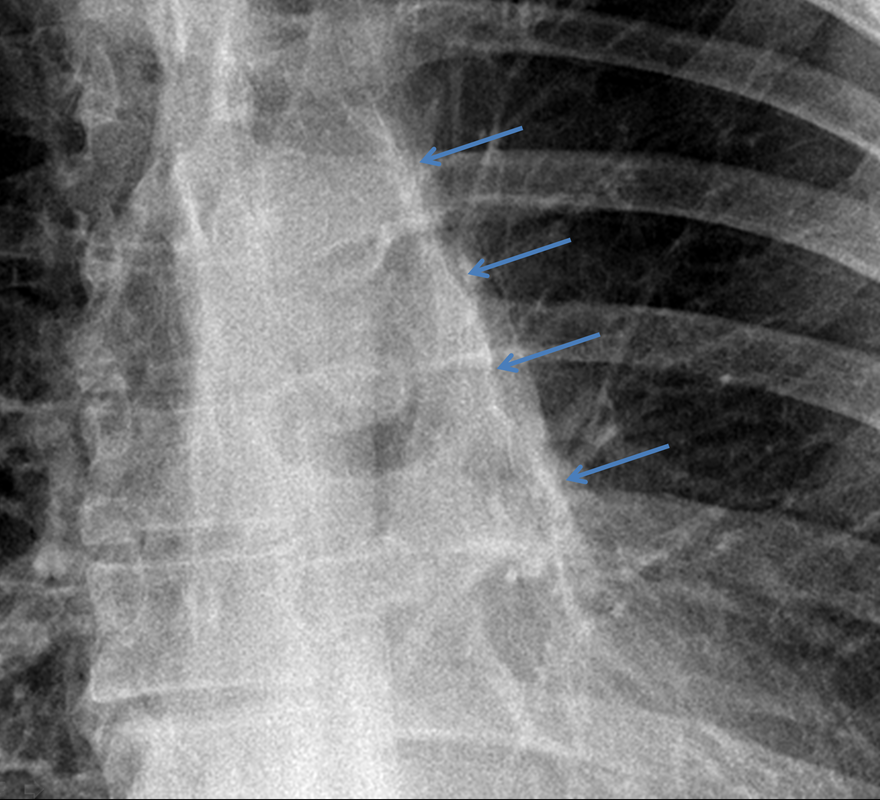 |
This case is a companion case to the Case 64, with many comparable features, many of which are more pronounced than the prior case. The left hemithorax is contracted with shift of both the superior and inferior mediastinum to the left. Comparable to the prior case there is also evidence of selective volume loss in the left upper thorax with elevation of the left hilar structures, a horizontal orientation of the left main bronchus and tenting of the left hemidiaphragm. However, in contradistinction to the prior case there is no perihilar opacity present. So this appears to reflect extreme left upper collapse but with no residual opacity visible to reflect the collapsed left upper lobe. There is an additional feature present. This is a fine line of high attenuation material running parallel to the mediastinal surface in the left perihilar region (arrow). The appearances are those of chain sutures as part of a left upper lobectomy which accounts for the volume loss differences demonstrated.
Lobectomy can be a difficult diagnosis to make. Appearances often mimic the characteristic appearances of lobar collapse but are lacking in the typical opacities that result from the collapsed lung parenchyma. Surgical clips are often conspicuous by their absence as these are rarely used or of a large enough size to be visualised on plain radiographs. Chain sutures can be variably used as in this case and be identified. These are used to complete an incomplete fissure and create a dividable plane so as to enable an air-leak free plane for an anatomical resection of the lobe. They can be difficult to see as they are so fine, resebling a very fine interlinked chain necklace. They are best visualised by magnification and sometime sharpening the image display. Post-operative changes of the ribs may also be appreciable, although this was more common in remote cases where a more extensive periosteal stripping was utilised that resulted in an irregular rib re- growth. In modern thoracotomy the rib irregularity is very focal and can be so subtle as to not even be identifiable even at CT. In post-lobectomy patients a small pleural effusion and persistent pleural thickening is often present at the lung bases, resulting in a long-standing pleural reaction. Determining the lobe of resection on plain radiographs relies on determining the position of the hilum and the central bronchovascular structures with expected superior displacement for upper lobe resections and conversely inferior displacement for lower lobe resections.
Lobectomy can be a difficult diagnosis to make. Appearances often mimic the characteristic appearances of lobar collapse but are lacking in the typical opacities that result from the collapsed lung parenchyma. Surgical clips are often conspicuous by their absence as these are rarely used or of a large enough size to be visualised on plain radiographs. Chain sutures can be variably used as in this case and be identified. These are used to complete an incomplete fissure and create a dividable plane so as to enable an air-leak free plane for an anatomical resection of the lobe. They can be difficult to see as they are so fine, resebling a very fine interlinked chain necklace. They are best visualised by magnification and sometime sharpening the image display. Post-operative changes of the ribs may also be appreciable, although this was more common in remote cases where a more extensive periosteal stripping was utilised that resulted in an irregular rib re- growth. In modern thoracotomy the rib irregularity is very focal and can be so subtle as to not even be identifiable even at CT. In post-lobectomy patients a small pleural effusion and persistent pleural thickening is often present at the lung bases, resulting in a long-standing pleural reaction. Determining the lobe of resection on plain radiographs relies on determining the position of the hilum and the central bronchovascular structures with expected superior displacement for upper lobe resections and conversely inferior displacement for lower lobe resections.
 RSS Feed
RSS Feed