
Radiology Level: FRCR, ABR, EDiR, MRCP, Radiology Senior +++
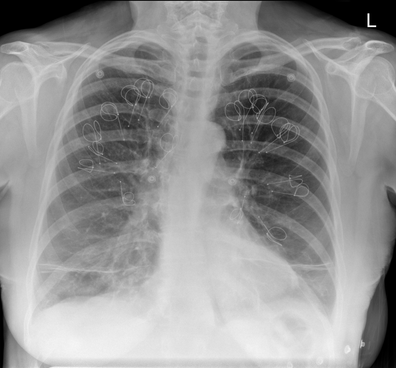
The appearances demonstrate multiple metallic loop structures in the upper lobes with extensive bibasilar atelectasis. These findings are due to endobronchial bronchoscopic insertion of nitinol endobronchial coils for the minimally invasive treatment of emphysema.
The principal of usage of these colis is that by reducing air flow to emphysematous diseased segments of lung, that there will be improved air fluid to more functional lung parenchyma and overall this will result in improved gas exchange and hence lung function. The procedure is intended to improve lung function patients with upper or lower lobe heterogeneous emphysema.
These endobronchial coils are inserted into the airways by bronchoscopy under sedation or general anaesthesia. A guide wire is inserted through the bronchoscope under fluoroscopic guidance. A catheter is passed over the guide wire and the straightened coil is introduced through the catheter with the catheter withdrawn as the coil held in place using grasper. When released the straightened coil reverts to to predetermined shape pulling the surrounding disease tissue and reducing lung volume. Usually up 5-15 coils are inserted per treated lobe (usually the upper lobes). Each lung is treated separately as there is a risk of pneumothorax. The coils remain permanently in location.
This type of volume reduction surgery is an alternative to patients undergoing formal lung volume reduction surgery or endobronchial valve insertion. The validity of such usage has been supported by small trials that suggest principally improved symptomatology, rather than measurable improved pulmonary function, after insertion versus control patients. The usage has been supported in the UK by NICE guidance.
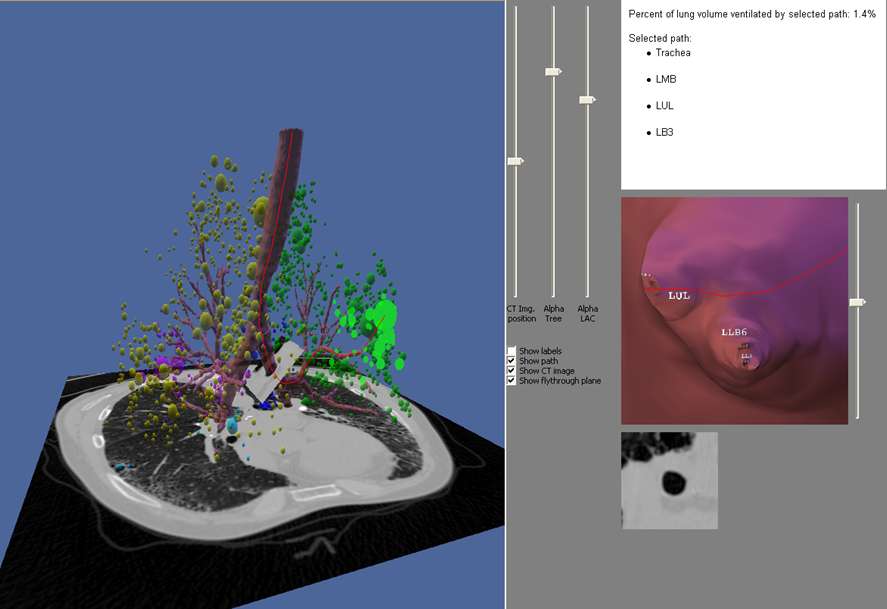
My entirely anecdotal experience, supported by radiological imaging is that this is entirely bogus! Emphysema at CT is either focal, or diffuse and heterogeneous. If it is focal and compressing normal lung, lung volume reduction surgery makes sense and I have seen real improvement. Endobronchial valves should theoretically work but tend in my experience to become obstructed by lung becoming atelectatic adjacent to them. Both these procedures can be supported by lung CT that specifically guides by virtual bronchoscopy to the areas to resect, or the particular airways to obstruct or bypass by a valve (see image below).
The principal of usage of these colis is that by reducing air flow to emphysematous diseased segments of lung, that there will be improved air fluid to more functional lung parenchyma and overall this will result in improved gas exchange and hence lung function. The procedure is intended to improve lung function patients with upper or lower lobe heterogeneous emphysema.
These endobronchial coils are inserted into the airways by bronchoscopy under sedation or general anaesthesia. A guide wire is inserted through the bronchoscope under fluoroscopic guidance. A catheter is passed over the guide wire and the straightened coil is introduced through the catheter with the catheter withdrawn as the coil held in place using grasper. When released the straightened coil reverts to to predetermined shape pulling the surrounding disease tissue and reducing lung volume. Usually up 5-15 coils are inserted per treated lobe (usually the upper lobes). Each lung is treated separately as there is a risk of pneumothorax. The coils remain permanently in location.
This type of volume reduction surgery is an alternative to patients undergoing formal lung volume reduction surgery or endobronchial valve insertion. The validity of such usage has been supported by small trials that suggest principally improved symptomatology, rather than measurable improved pulmonary function, after insertion versus control patients. The usage has been supported in the UK by NICE guidance.
My entirely anecdotal experience, supported by radiological imaging is that this is entirely bogus! Emphysema at CT is either focal, or diffuse and heterogeneous. If it is focal and compressing normal lung, lung volume reduction surgery makes sense and I have seen real improvement. Endobronchial valves should theoretically work but tend in my experience to become obstructed by lung becoming atelectatic adjacent to them. Both these procedures can be supported by lung CT that specifically guides by virtual bronchoscopy to the areas to resect, or the particular airways to obstruct or bypass by a valve (see image below).
In contradistinction these valves may I am sure help the occasional patient who has diffuse emphysema in the upper lobes, by reducing ventilation and perfusion to these areas. But for most people with "heterogeneous emphysema" on CT have a bulla here and a bulla there throghout the lungs. Randomly inserting some coils is just as likely to reduce ventilation and perfusion to a good subsegment of lung as to an emphysematous portion.
It, therefore, comes to me as no surprise that a recent large study in JAMA casts doubt even on the symptom based improvement of these devices (6 minute walks, questionairres), suggesting much of this must be placebo related. Importantly it states that the treated groups unsurprsingly suffer considerably more pneuthoraces and infective exacerbations.
Regardless these will be around for a while and need to be recognised. This patient suffered from recurrent haemoptysis, likely due the coils.
Reference:
Sciurba FC et al. JAMA. 2016 May 24-31;315(20):2178-89. doi: 10.1001/jama.2016.6261.
Effect of Endobronchial Coils vs Usual Care on Exercise Tolerance in Patients With Severe Emphysema: The RENEW Randomized Clinical Trial.
https://www.ncbi.nlm.nih.gov/pubmed/27179849
It, therefore, comes to me as no surprise that a recent large study in JAMA casts doubt even on the symptom based improvement of these devices (6 minute walks, questionairres), suggesting much of this must be placebo related. Importantly it states that the treated groups unsurprsingly suffer considerably more pneuthoraces and infective exacerbations.
Regardless these will be around for a while and need to be recognised. This patient suffered from recurrent haemoptysis, likely due the coils.
Reference:
Sciurba FC et al. JAMA. 2016 May 24-31;315(20):2178-89. doi: 10.1001/jama.2016.6261.
Effect of Endobronchial Coils vs Usual Care on Exercise Tolerance in Patients With Severe Emphysema: The RENEW Randomized Clinical Trial.
https://www.ncbi.nlm.nih.gov/pubmed/27179849
 RSS Feed
RSS Feed