
Radiology Level: FRCR, FRCS, MRCP, ABR, EDiR, Radiology Junior +
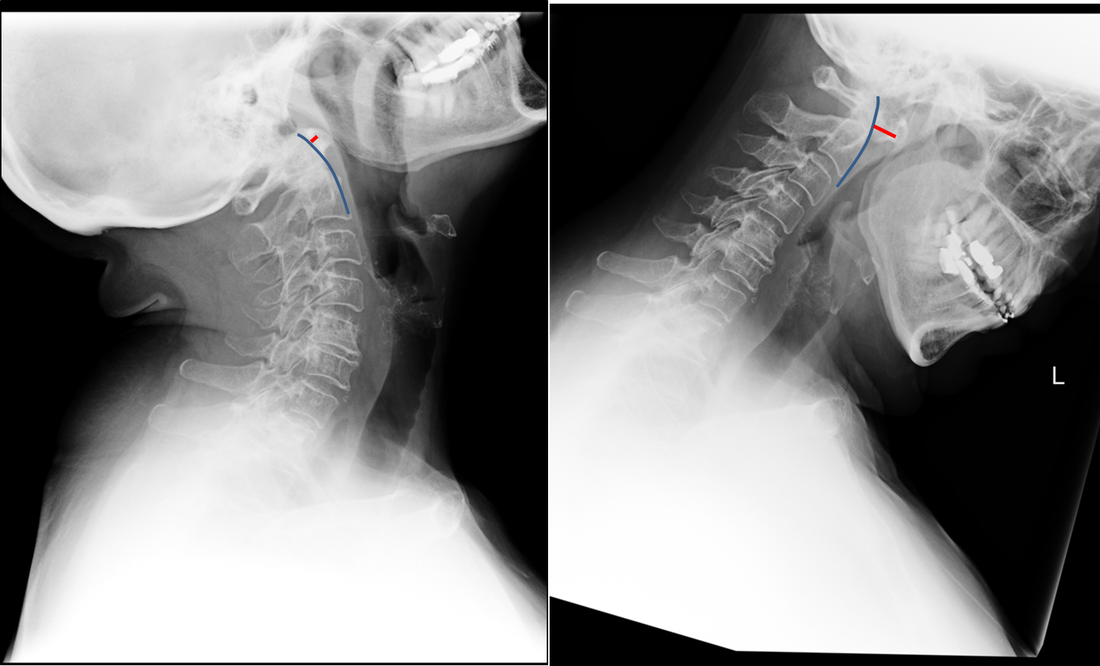
The images demonstrate a pair of cervical spine radiographs. The image on the left is in extension the image on the right in flexion. Both images are adequate visualising to C7-T1 or lower. The extension image demonstrates that there is some moderate degenerative change with sclerosis and joint space reduction at C5-C6. The flexion film demonstrates that there is straightening of the cervical spine at this level in flexion. There is, however, no spondylolisthesis (slip).
Looking more carefully at the atlanto (C1) –axial (C2) articulation, we can see that in extension the anterior margin of the dens can be traced superiorly to the skull base (blue line). The predental space (also called atlantodental or predentate space) measures only 2mm (red line). In flexion though the predental space greatly increases to >7mm. The appearances are those of non-traumatic atlanto-axial subluxation/dislocation. In addition there is some loss of clarity of the odontoid peg (confirmed on MRI/CT) suggesting some erosion. These appearances were due to rheumatoid disease. The patient was being assessed pre-operatively.
Typically the predental space is usually <=3mm in neutral or extension radiographs, <=5mm in children. In children the ligamentous laxity of the neck in flexion allows some minor increase of this space, but not in adults. The anterior motion of the atlas on the axis/dens is typically restricted by the transverse ligament. The disruption of this ligament can occur by trauma (look for associated fractures or prevertebral soft tissue swelling) or by inflammatory conditions (typically rheumatoid disease but also less commonly psoriasis, Down’s and Morquio’s syndromes, Neurofibromatosis, Osteogenesis Imperfecta).
Disruption of the transverse ligament enables atlanto-axial instability. This can be asymptomatic or life-threatening (particularly in trauma). Specifically, posterior translation of the dens can compress the cord resulting in upper motor neuron compressive neurology. Such unexpected spinal compression may become first apparent during intubation and is, therefore, screened for in susceptible patients with rheumatoid arthritis. The condition is termed atlanto-axial instability/subluxation or dislocation and should be differentiated from atlanto-axial rotatory subluxation in which the primary injury is a rotation at C1-C2 that may be associated with unilateral facet dislocation, fractures and nerve root compression with flexed rotated angulated neck malalignment.
Looking more carefully at the atlanto (C1) –axial (C2) articulation, we can see that in extension the anterior margin of the dens can be traced superiorly to the skull base (blue line). The predental space (also called atlantodental or predentate space) measures only 2mm (red line). In flexion though the predental space greatly increases to >7mm. The appearances are those of non-traumatic atlanto-axial subluxation/dislocation. In addition there is some loss of clarity of the odontoid peg (confirmed on MRI/CT) suggesting some erosion. These appearances were due to rheumatoid disease. The patient was being assessed pre-operatively.
Typically the predental space is usually <=3mm in neutral or extension radiographs, <=5mm in children. In children the ligamentous laxity of the neck in flexion allows some minor increase of this space, but not in adults. The anterior motion of the atlas on the axis/dens is typically restricted by the transverse ligament. The disruption of this ligament can occur by trauma (look for associated fractures or prevertebral soft tissue swelling) or by inflammatory conditions (typically rheumatoid disease but also less commonly psoriasis, Down’s and Morquio’s syndromes, Neurofibromatosis, Osteogenesis Imperfecta).
Disruption of the transverse ligament enables atlanto-axial instability. This can be asymptomatic or life-threatening (particularly in trauma). Specifically, posterior translation of the dens can compress the cord resulting in upper motor neuron compressive neurology. Such unexpected spinal compression may become first apparent during intubation and is, therefore, screened for in susceptible patients with rheumatoid arthritis. The condition is termed atlanto-axial instability/subluxation or dislocation and should be differentiated from atlanto-axial rotatory subluxation in which the primary injury is a rotation at C1-C2 that may be associated with unilateral facet dislocation, fractures and nerve root compression with flexed rotated angulated neck malalignment.
 RSS Feed
RSS Feed